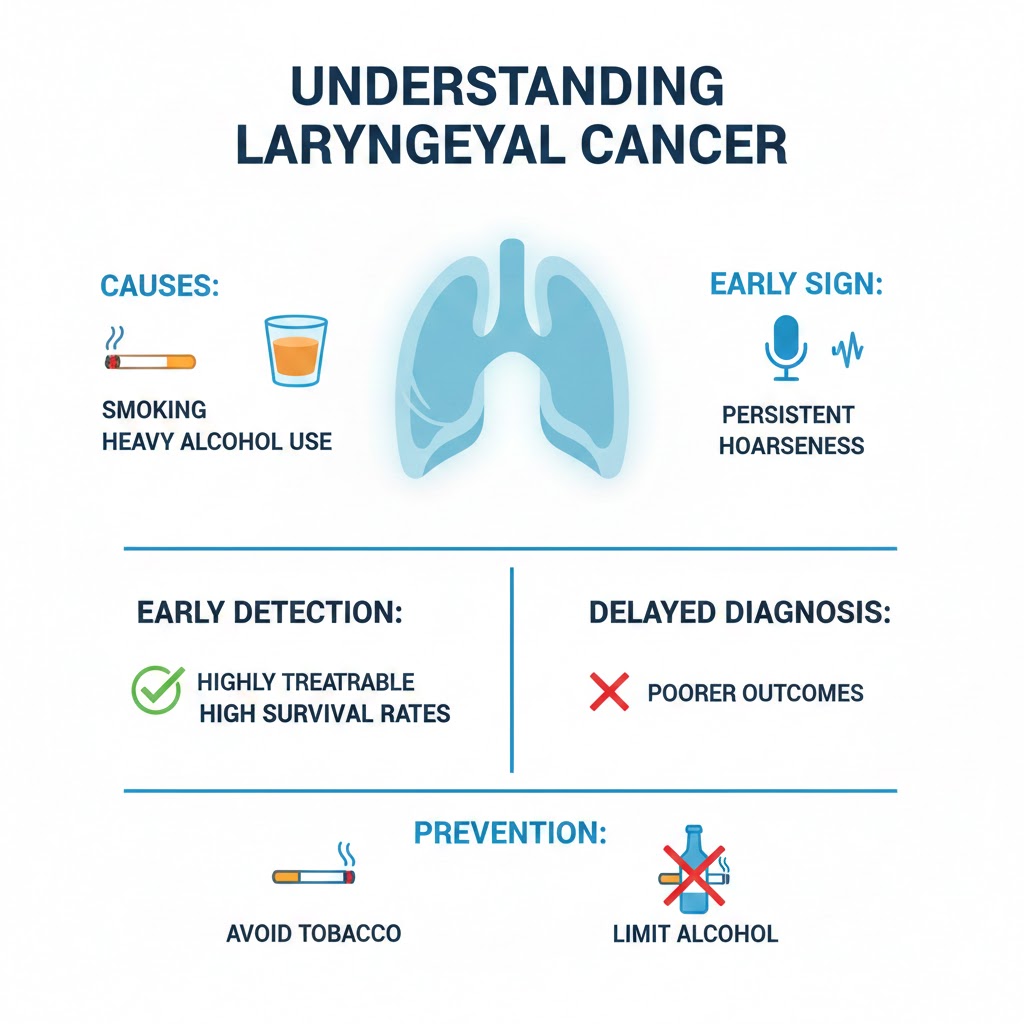
Laryngeal cancer affects the voice box and is most often caused by smoking and heavy alcohol use. Persistent hoarseness is the most common early sign, along with throat discomfort or difficulty swallowing. When detected early, the disease is highly treatable and survival rates are high; outcomes are poorer when diagnosis is delayed. Prevention through avoiding tobacco and excessive alcohol, and prompt medical attention for lasting voice changes, are key to saving lives.
Laryngeal cancer affects a vital organ: the larynx, often called the voice box. Located at the top of the windpipe, the larynx plays a central role in breathing, speaking, and swallowing. When cancer develops there, it can profoundly alter daily life, sometimes in ways that are both visible and audible.
Laryngeal cancer is far more common in men than in women, a difference that largely reflects patterns of tobacco and alcohol use. The disease is usually diagnosed after the age of 50, though cases in younger people are not unheard of.
The causes of laryngeal cancer are well established. Tobacco is by far the leading risk factor. Cigarettes, cigars, pipes, and even some smokeless tobacco products expose the lining of the larynx to carcinogenic substances that, over time, can trigger malignant changes. Alcohol acts as a powerful accomplice: heavy drinking combined with smoking multiplies the risk. Other factors can also play a role, including occupational exposure to certain chemicals, such as asbestos or wood dust. Infection with the human papillomavirus, better known for its link to cervical cancer, has also been implicated in a subset of cases.
Because the main causes are known, prevention is straightforward. Avoiding tobacco dramatically reduces the risk, and the benefits begin soon after quitting. Limiting alcohol consumption adds further protection. Workplace safety measures that reduce exposure to harmful fumes and dusts matter as well.
The first signs of the disease are often subtle, which explains why diagnosis can be delayed. Persistent hoarseness is the most common warning sign, especially when it lasts longer than a few weeks and has no obvious cause. A sore throat that does not go away, difficulty or pain when swallowing, a sensation of a lump in the throat, chronic cough, or ear pain can also be clues. In more advanced stages, breathing may become difficult, or a mass may be felt in the neck due to spread to nearby lymph nodes.
When such symptoms raise suspicion, diagnosis usually begins with a careful examination of the throat by an ear, nose, and throat specialist. Using a small camera passed through the nose or mouth, the doctor can visualize the larynx directly. If an abnormal area is seen, a biopsy is required to confirm the presence of cancer. Imaging tests such as CT scans, MRI, or PET scans help determine how far the disease has spread, information that is crucial for choosing the best treatment.
The course of laryngeal cancer varies widely. Tumors confined to the vocal cords tend to be detected earlier, because even small lesions can affect the voice. These early-stage cancers generally have an excellent prognosis. Cancers that arise above or below the vocal cords may grow larger before causing symptoms and are therefore more often diagnosed at a later stage. Over time, untreated cancer can invade nearby tissues or spread to lymph nodes and distant organs, making treatment more complex and outcomes less favorable.
Treatment depends on the stage of the disease, the exact location of the tumor, and the patient’s overall health. For early cancers, radiation therapy or limited surgery can often eliminate the tumor while preserving the voice. More advanced cases may require a combination of surgery, radiotherapy, and chemotherapy. In some situations, part or all of the larynx must be removed to control the disease, a life-saving operation that has profound consequences for speech and breathing. Advances in reconstructive surgery, voice rehabilitation, and assistive technologies have greatly improved quality of life for people who undergo such procedures.
Survival rates reflect this wide spectrum of disease. When laryngeal cancer is diagnosed at an early stage, five-year survival can exceed 80 or even 90 percent. For cancers detected later, especially those that have spread beyond the larynx, survival drops significantly, often to around 40 percent or less. These figures underscore a simple but crucial message: early detection saves lives.
Laryngeal cancer is a disease in which prevention, awareness of symptoms, and timely medical attention make a tangible difference.
Use the ‘Comments’ field below to share your experience with larynx cancer or to suggest improvements to this article.