Smoking is notorious for its role in lung cancer, but its impact on the mouth and throat is often underestimated. Cancer of the oral cavity, which includes the lips, tongue, gums, floor of the mouth, and palate, is a serious disease whose primary cause remains tobacco smoking
Who is Affected:
Tobacco use is by far the most significant risk factor for oral cancer. The risk for a person who smokes can be multiplied by five or more compared to someone who has never touched tobacco. This correlation applies not only to cigarettes but also to cigars and pipes.
It is crucial to emphasize, however, that oral cancer is not exclusively a smoker’s disease. A significant percentage of cases occur in individuals who have never smoked. These cases are often linked to other risk factors, notably alcohol use and infection with the Human Papillomavirus (HPV). The combined effect of alcohol and tobacco is strongly synergistic, multiplying the risk exponentially.
The Mechanism of the Disease
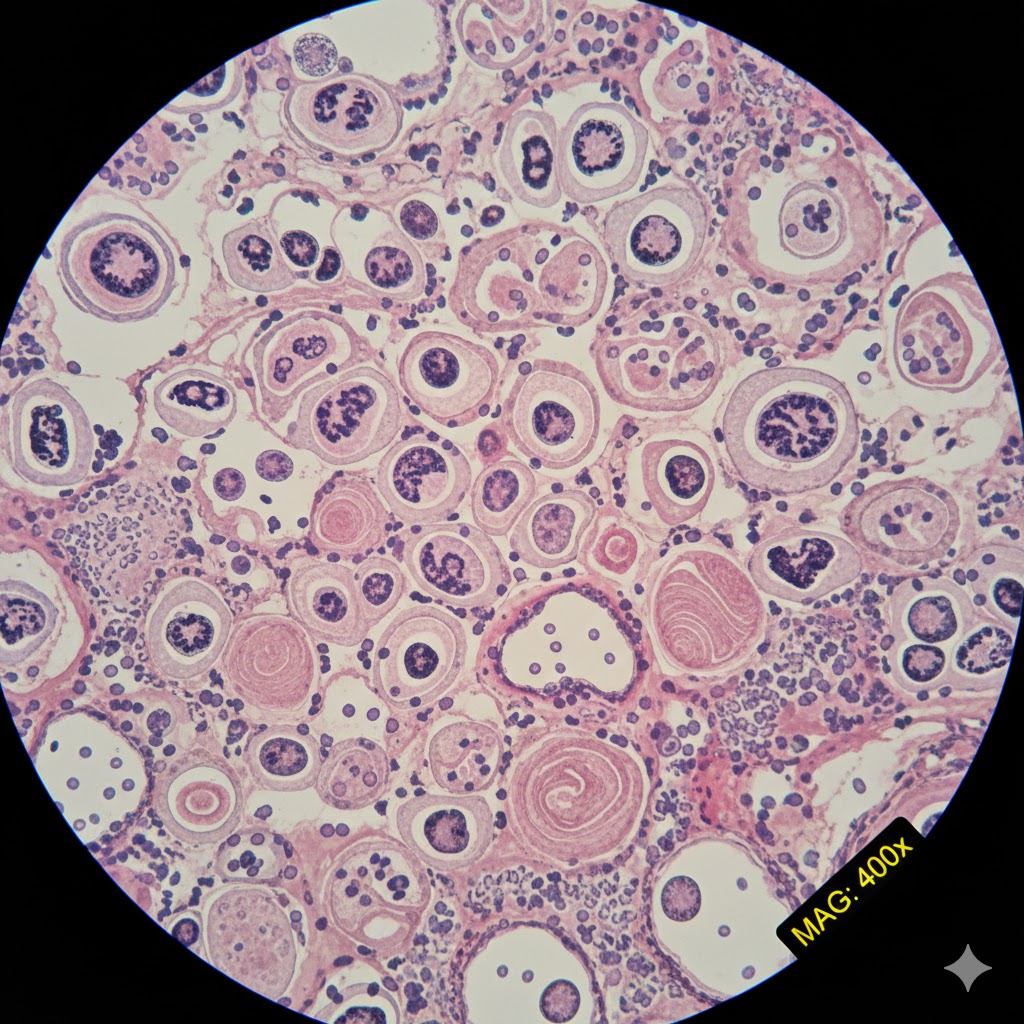
The reason tobacco smoke triggers oral cancer lies in its chemical composition. Tobacco smoke contains thousands of chemical substances, dozens of which are known carcinogens. When these compounds come into contact with the delicate tissues of the mouth, they attack the DNA of the epithelial cells. These toxic substances cause genetic mutations which, over time and with repeated exposure, disrupt the normal mechanisms of cell growth and division. The mutated cells then begin to multiply uncontrollably, forming precancerous lesions, such as leukoplakia (white patch) or erythroplakia (red patch), which can progress to squamous cell carcinoma, the most common form of oral cancer. The chronic inflammation induced by tobacco only worsens this carcinogenic process.
Signs, Diagnosis, and Treatment
Oral cancer, if detected early, offers excellent chances of cure. The problem lies in the fact that the initial symptoms are often subtle or mistaken for benign conditions.
The symptoms to watch out for are:
A sore or ulcer in the mouth or on the lip that does not heal after two weeks.
The appearance of a persistent white, red, or mixed patch on the oral lining or tongue.
A thickening, lump, or nodule in the cheek or neck.
Unexplained pain, numbness, or bleeding in the mouth.
Difficulty chewing, swallowing, or moving the tongue.
The diagnosis begins with a thorough clinical examination, often performed by a dentist or physician. Any persistent suspicious lesion requires a biopsy, which involves taking a small sample of tissue for laboratory analysis. If cancer is confirmed, imaging tests (CT scan, MRI, PET scan) are performed to determine the extent of the tumor and to check whether it has reached the lymph nodes in the neck or other parts of the body, or whether the cancer has spread to other organs (metastasis).
Treatment depends on the stage and location of the cancer. It most often involves a combination of:
Surgery to remove the tumor and, if necessary, the affected lymph nodes.
Radiation therapy to destroy remaining cancer cells.
Chemotherapy or immunotherapy in more advanced cases or to increase the effectiveness of other treatments.
Prognosis and the Importance of Quitting
The prognosis is directly related to the stage of the cancer at the time of diagnosis. When the disease is localized and detected very early, the five-year survival rate is significantly higher. Unfortunately, many cases are diagnosed at an advanced stage, when the cancer has spread to the lymph nodes, which makes treatment more arduous and significantly reduces the chances of recovery.
The most powerful impact on the prognosis lies in the immediate and definitive cessation of tobacco use, even after diagnosis. Quitting smoking not only reduces the risk of recurrence but also improves the response to treatments and the overall quality of life of the patient. Prevention remains the most effective weapon: avoiding tobacco and excessive alcohol use are the fundamental steps to guard against this devastating disease.
Use the ‘Comments’ field below to share your experience with oral cancer or to suggest improvements to this article.
Smoking has direct and devastating effects on the mouth, starting with colored teeth and bad breath, progressing to tooth decay, and potentially leading to cancer.
Why Smoking and Oral Disease Are Linked
The link between smoking and oral health problems stems from the thousands of toxic chemicals found in tobacco smoke. When these chemicals enter the mouth, they disrupt its natural defenses and processes. Nicotine, carbon monoxide, tar, and various carcinogens in cigarettes irritate soft tissues, impair blood circulation, weaken the immune system, and promote the proliferation of harmful bacteria.
Smoking restricts the flow of oxygen and nutrients to the gums and bone, impairing the mouth’s ability to heal and fight off infections. It also changes the composition of saliva, making it less effective at neutralizing acids and washing away food particles and bacteria. This combination of factors creates a hostile environment where oral diseases can flourish, often with greater severity and resistance to treatment.
Dental Problems: Beyond the Stain
The most visible sign of a smoker’s habit is often the yellowish or brownish stains on their teeth, a direct result of tar accumulating on the enamel. However, the damage goes far deeper than aesthetics. Smoking significantly increases the risk of dental caries, or cavities. The altered oral environment, with reduced saliva flow and a shift towards more acid-producing bacteria, creates ideal conditions for tooth decay.
Furthermore, smokers are at a much higher risk for oral cancer. The carcinogens in tobacco smoke directly damage the cells lining the mouth, tongue, lips, throat, and salivary glands, leading to abnormal cell growth. These cancers often present as persistent sores, lumps, or white/red patches that don’t heal, and early detection is critical for survival.
Periodontal Problems: The Foundation Crumbles
Perhaps one of the most insidious effects of smoking is its impact on periodontal health, which refers to the gums and the bone supporting the teeth. Smokers are at a significantly elevated risk for gingivitis (inflammation of the gums) and, more severely, periodontitis.
Smoking masks the classic signs of gum disease. Nicotine constricts blood vessels, meaning smokers often experience less bleeding gums, even when severe inflammation is present. This can lull them into a false sense of security, delaying diagnosis and treatment until the disease has advanced. By the time it’s noticeable, the damage can be extensive.
Periodontitis in smokers progresses more rapidly and is often more severe than in non-smokers. It leads to the destruction of the bone and connective tissues that hold teeth in place, eventually resulting in loose teeth and, ultimately, tooth loss. Smokers also respond less favorably to periodontal treatments and are more prone to recurrence of the disease.
Bad Breath: A Lingering Consequence
Halitosis, commonly known as bad breath, is another prevalent issue among smokers. The lingering smell of stale tobacco smoke itself is a primary contributor. However, the problem is compounded by the drying effect of smoke on the mouth, leading to reduced saliva flow and an increase in odor-producing bacteria. Periodontal disease, also exacerbated by smoking, further contributes to halitosis, as decaying tissue and bacterial buildup release unpleasant sulfur compounds.
Diminished Senses of Taste and Smell: A Muted World
Smoking dulls the senses of taste and smell. The chemicals in tobacco smoke can damage the taste buds and interfere with the olfactory receptors in the nose. Smokers often report that food tastes bland or that they struggle to discern subtle flavors. This reduced sensory perception can diminish the enjoyment of eating and drinking, and for some, it even contributes to unhealthy dietary choices as they seek stronger-tasting foods.
Dry Mouth: A Gateway to Further Issues
Xerostomia, or dry mouth, is a common complaint among smokers. The heat and chemicals in cigarette smoke irritate the salivary glands and can reduce saliva production. Saliva is crucial for oral health; it washes away food particles, neutralizes acids, helps remineralize tooth enamel, and contains antimicrobial agents. A chronically dry mouth leaves individuals more susceptible to cavities, gum disease, fungal infections (like thrush), and difficulty speaking or swallowing.
Safeguarding Your Smile: Oral Hygiene Advice
The most impactful advice for anyone concerned about their oral health and smoking is unequivocal: quit smoking. Cessation immediately begins to reverse many of the damaging effects and significantly reduces the risk of developing further complications.
Beyond quitting, meticulous oral hygiene practices are essential for smokers and former smokers:
Brush thoroughly twice a day: Use a soft-bristled brush and fluoride toothpaste to gently clean all tooth surfaces and along the gumline.
Floss daily: Flossing removes plaque and food particles from between teeth and under the gumline, areas a toothbrush cannot reach.
Regular dental check-ups and cleanings: Visit your dentist at least twice a year, or more frequently if advised, for professional cleanings and examinations. Your dentist can monitor for early signs of oral cancer, gum disease, and other problems.
Use an antimicrobial mouthwash: A therapeutic mouthwash can help reduce bacteria in the mouth.
Stay hydrated: Drinking plenty of water helps combat dry mouth and encourages saliva production.
Maintain a balanced diet: Limit sugary and acidic foods and drinks that can contribute to tooth decay.
Be vigilant for changes: Any persistent sore, lump, patch, or unusual bleeding in your mouth should be reported to your dentist immediately.
Use the ‘Comments’ field below to share your experience or to suggest improvements to this article.
The public debate surrounding smoking has legitimately focused on its physical ravages: cancer, heart disease, and lung disease. However, smoking harbors a more subtle but equally serious danger: its complex and harmful link to mental health, particularly depression. Smoking is deeply linked to emotional well-being, often acting as a treacherous coping mechanism that ultimately exacerbates the disorders it is supposed to alleviate.
The Scientific Evidence for this Association
Extensive research, spanning large epidemiological studies and clinical trials, has firmly established a reciprocal link between smoking and depressive disorders. The evidence points not to a coincidence, but to a powerful, two-way street that traps individuals in a vicious cycle.
First, the scientific data shows that people suffering from depression are significantly more likely to smoke. They often start smoking at a younger age, smoke more heavily, and are less likely to successfully quit compared to the general population. The act of lighting up may be an attempt to self-medicate or manage the intense negative feelings and low energy characteristic of depression.
Second, the relationship is bidirectional: long-term, heavy smoking itself appears to increase the risk of developing future depressive episodes. While nicotine initially offers a perceived “lift” or temporary calming effect, the long-term impact on brain chemistry is destabilizing, setting the stage for emotional volatility and mood disorders.
Finally, and perhaps most critically for those seeking recovery, quitting smoking can sometimes trigger a depressive episode. This cessation-related depression is a recognized withdrawal symptom, highlighting just how deeply the brain has adapted to and become dependent on nicotine for mood regulation.
The Biological Mechanisms Driving the Association
Understanding this complex link requires looking inside the brain, where the primary players are nicotine and the neurotransmitter systems that govern mood.
Dopamine: Nicotine is a psychoactive drug that rapidly reaches the brain and stimulates the release of dopamine—often called the “reward” chemical. This surge produces immediate feelings of pleasure, focus, and reduced stress, offering a quick but fleeting high that can mask depressive symptoms. Smokers, especially those with existing depression, begin to rely on this nicotine-induced dopamine hit to temporarily elevate their mood. However, the brain eventually adjusts by reducing its natural production of dopamine and the sensitivity of its own receptors. This process, called tolerance, means the smoker needs more nicotine just to feel normal, and when they are not smoking, their mood baseline sinks even lower than it was before they started. This neurological dependency exacerbates existing depression.
Chronic Stress and Inflammation: Long-term smoking is associated with chronic inflammation throughout the body and brain. This persistent inflammatory state has been strongly implicated in the pathology of major depressive disorder. Furthermore, many of the toxic components of tobacco smoke stress the body, disrupting the hypothalamic-pituitary-adrenal (HPA) axis—the body’s main stress response system—leaving the individual less resilient to psychological stress and more prone to mood disturbances.
Monoamine Oxidase (MAO) Inhibition: Tobacco smoke contains chemicals that act as monoamine oxidase inhibitors. MAO is an enzyme that breaks down key mood-regulating neurotransmitters like dopamine, serotonin, and norepinephrine. By inhibiting MAO, smoking artificially increases the levels of these neurotransmitters in the short term, again contributing to a temporary mood boost. When a person quits, this pharmacological effect vanishes, and the sudden drop in these neurotransmitters contributes directly to the mood disturbance and depression experienced during withdrawal.
Preventive Measures and Supportive Interventions
Given this deeply intertwined relationship, the strategies for reducing the harms must address both the nicotine addiction and the underlying mental health condition simultaneously.
For Depressed Individuals (Prevention of Smoking):
Healthcare providers must actively screen patients with mood disorders for smoking risk. Prevention efforts should focus on effective coping strategies that do not involve substances. Integrating behavioral therapy and antidepressant medication early in the treatment of depression can reduce the urge to use smoking as a self-medicating tool. Public health messages need to explicitly counter the common misconception that smoking is an effective stress reliever, clarifying its role as a mood destabilizer.
For Smokers (Successful Cessation and Relapse Prevention):
For current smokers, particularly those with a history of depression, quitting requires a specialized approach.
Pharmacological Support: Using pharmacotherapies for smoking cessation, such as nicotine medications, varenicline or bupropion (an antidepressant often used for cessation), is particularly important. These medications can ease withdrawal symptoms, reduce cravings, and, in the case of bupropion, help mitigate the depressive symptoms that can occur upon quitting.
Integrated Behavioral Therapy: Cessation programs for this group must be dual-purpose, treating both the addiction and providing mental health coping skills. Smokers need psychological support to anticipate and manage the temporary period of low mood during withdrawal, recognizing it as a transient physical symptom rather than a relapse of their underlying depression.
Close Monitoring: Healthcare providers must closely monitor the patient’s mood during the initial weeks of quitting. If significant depressive symptoms emerge, it is crucial to intervene quickly with intensified counseling or, potentially, the short-term use of antidepressant medications to prevent a relapse back to smoking.
For many people, the dangers of smoking are understood primarily in terms of long-term conditions like cancer and heart disease. Yet, one of the most immediate and pervasive negative impacts of tobacco use—its destructive effect on the body’s natural healing process—often remains less known until a medical procedure makes it acutely relevant. Smoking severely compromises the biological mechanisms required to mend tissue, turning what should be a straightforward recovery into a risky and drawn-out ordeal.
The Biological Causes
The connection between smoking and poor wound healing is not anecdotal; it is firmly rooted in cellular biology and physiology. The harmful chemicals found in tobacco and cigarette smoke create several major roadblocks that impede the body’s repair efforts:
Impaired Oxygen Delivery (Hypoxia): The most critical factor is the presence of carbon monoxide, a gas inhaled with tobacco smoke. Carbon monoxide bonds tightly to hemoglobin in red blood cells, effectively displacing oxygen. This reduces the blood’s capacity to carry oxygen to tissues throughout the body, including the site of an injury or surgical incision. Wounds require vast amounts of oxygen to fuel the rapid cell division, collagen synthesis, and immune response needed for healing. Without sufficient oxygen, the cells simply cannot perform their repair functions efficiently.
Vasoconstriction: Nicotine causes blood vessels to constrict (narrow). This action immediately reduces blood flow, further starving the injured tissue of both oxygen and vital nutrients, such as proteins and vitamins, necessary for repair. This is especially problematic in the fine, delicate capillary beds near the skin’s surface where most surgical wounds are closed.
Compromised Immune Function: Smoking affects the activity of key immune cells, particularly white blood cells called neutrophils and macrophages, which are the body’s first line of defense against infection. When these cells are weakened, the wound site is less able to fight off bacteria, significantly raising the risk of infection.
Disruption of Collagen Synthesis: Collagen is the crucial structural protein that forms the scaffolding of new tissue. Smoking interferes with the activity of fibroblasts, the cells responsible for manufacturing collagen. This results in weaker, less organized, and less resilient scar tissue, increasing the likelihood that the incision will break down or fail to close properly.
Scientific Evidence Across Common Operations
The impact of these biological mechanisms is clearly documented in surgical outcomes across various medical specialties. The data consistently demonstrates that smokers experience higher rates of complications compared to non-smokers following common procedures.
Orthopedic Surgery: In operations like spinal fusion or fracture repair, bone healing is paramount. Smoking is known to significantly increase the risk of non-union, where the bone fails to fuse properly. This risk can be two to three times higher in smokers. The reduced blood flow inhibits the delivery of bone-building cells and oxygen needed for ossification.
General and Abdominal Surgery: Following procedures such as hernia repair or bowel surgery, smokers face dramatically higher rates of surgical site infection (SSI) and wound dehiscence (the splitting open of a wound along the surgical suture). The combination of poor circulation and a weakened immune system creates a fertile ground for bacteria.
Plastic and Reconstructive Surgery: Surgeons in this field often rely on the viability of highly vascularized tissue flaps. Smoking is a significant contraindication because the vasoconstrictive effects of nicotine and lack of oxygen can cause the edges of the flap to die (necrosis), leading to tissue loss and catastrophic surgical failure.
Dental and Periodontal Surgery: Even minor oral procedures, such as tooth extractions or gum grafts, show impaired healing. Smoking is a primary risk factor for dry socket and contributes to the failure of dental implants because the surrounding bone and gum tissue cannot integrate with the foreign material effectively.
The Consequences of Impaired Healing
The outcome of smoking-related healing problems extends far beyond a simple delay in recovery. The consequences are often severe and have substantial medical and financial ramifications:
Increased Infection and Readmission: Poorly oxygenated, compromised wounds are far more likely to become infected, requiring aggressive antibiotic treatment, repeat debridement (removal of dead tissue), and, critically, often lead to an expensive and distressing hospital readmission.
Scarring and Functional Deficits: The interference with collagen production means that when a wound does finally close, the scar is often weaker, wider, and cosmetically poorer. In orthopedic cases, failed fusion or poor tendon repair can lead to long-term functional disability and chronic pain.
Failed Procedures and Repeat Surgeries: When bone grafts, skin flaps, or other reconstructive elements fail due to necrosis or non-union, the patient often faces the physical and emotional toll of needing multiple revision surgeries, which themselves carry escalating risks.
Preventive Measures
The good news is that the negative effects of smoking on healing are largely reversible, making prevention and preoperative intervention the most powerful tools surgeons and patients possess.
The single most effective and necessary preventive measure is smoking cessation. The benefits of quitting begin almost immediately. Within twenty-four hours, the carbon monoxide levels in the blood drop, restoring the blood’s oxygen-carrying capacity. Within days or weeks, the function of the immune cells improves, and circulation begins to normalize as the acute effects of nicotine wear off.
Most medical guidelines recommend that patients planning any significant elective surgery stop smoking completely at least four to six weeks before the operation and remain abstinent for at least four to six weeks post-operatively. This window is generally deemed the minimum time required to normalize many of the key physiological healing pathways. Shorter periods of abstinence are still beneficial, but the full four-to-six-week period is ideal for minimizing risk.
Healthcare providers often play a crucial role by screening all patients for tobacco use and strongly recommending and facilitating specialized cessation programs that utilize a combination of counseling, behavioral therapy, and pharmacological aids like nicotine replacement therapy (NRT). While NRT products still deliver nicotine, they eliminate the carbon monoxide and thousands of other toxins found in smoke, offering a safer alternative during the critical pre- and post-operative period.
Smoking is one of the leading preventable factors contributing to premature death and disabling illness worldwide. Despite decades of public health action and widespread awareness of its dangers, the number of smoking-related deaths remains staggering.
The Staggering Scale of Death
Across the globe, smoking is responsible for a monumental loss of life. The World Health Organization (WHO) estimates that tobacco claims more than eight million lives annually. The vast majority—over seven million—result from direct tobacco use, while approximately 1.2 million fatalities occur among non-smokers exposed to secondhand smoke. This positions tobacco as one of the pre-eminent preventable causes of death internationally.
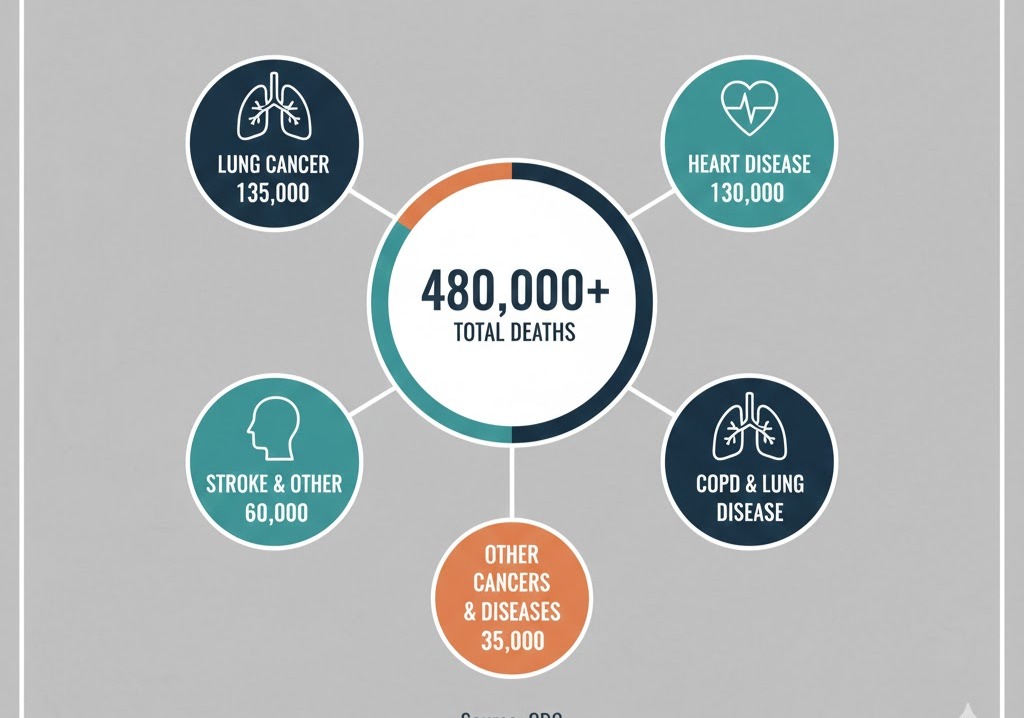
United States: U.S. health authorities, including the Centers for Disease Control and Prevention (CDC), state that smoking accounts for over 480,000 deaths each year in the nation, a figure that includes victims of secondhand smoke. This means that roughly one in five deaths is attributable to smoking. Remarkably, this total surpasses the combined mortality from HIV, illegal drug use, excessive alcohol consumption, traffic accidents, and firearm injuries.
United Kingdom: In the UK, data from the National Health Service (NHS) and related agencies indicates that smoking leads to around 76,000 deaths annually. This constitutes about fifteen percent of all deaths among adults aged thirty-five and older, demonstrating its substantial drain on public health.
Comparing Smoking Versus Other Major Risks
To properly assess the immense impact of smoking, a comparison with other major public health threats is necessary:
Overweight and Obesity: While excess weight and obesity pose serious threats, contributing to conditions such as heart disease, diabetes, and certain malignancies, direct mortality figures are intricate to isolate. Nonetheless, studies consistently demonstrate that tobacco smoking is a more direct and potent killer than obesity alone. In many analyses, the number of deaths directly caused by smoking far exceeds those directly linked to obesity, although it is important to acknowledge that obesity exacerbates chronic diseases and often compounds the risks associated with smoking.
Alcohol: Alcohol misuse is another significant source of preventable death, resulting in fatalities from liver failure, accidents, violent incidents, and specific cancers. Although alcohol-related deaths are substantial—estimated by the WHO at roughly three million globally each year—the total worldwide mortality caused by tobacco typically remains higher. Both in the US and the UK, while alcohol-related deaths are a critical concern, they generally do not reach the devastating overall numbers associated with smoking.
This comparison emphasizes that while the problems of excess weight and alcohol consumption are vital public health priorities, smoking occupies a uniquely destructive position as a powerful and singular cause of early mortality.
The Main Diseases Responsible for Smoking-Related Mortality
Smoking does not attack a single target; it harms virtually every bodily system, resulting in a broad spectrum of fatal illnesses. The primary contributors to smoking-related mortality include:
Cardiovascular Diseases: This category is the leading cause of death among smokers. Smoking drastically increases the likelihood of heart attack, stroke, coronary artery disease, peripheral artery disease, and aneurysm. Toxic chemicals in tobacco damage blood vessel linings, accelerate the accumulation of arterial plaque, and elevate blood pressure and heart rate.
Cancers: Smoking is a direct cause of cancer in almost all areas of the body. Lung cancer is the most recognized consequence, with approximately ninety percent of lung cancer deaths stemming from smoking. However, tobacco also causes cancers of the mouth, throat (pharynx), voice box (larynx), esophagus, stomach, colon, rectum, liver, pancreas, kidney, bladder, cervix, and a specific type of blood cancer (acute myeloid leukemia).
Chronic Obstructive Pulmonary Disease (COPD): This broad diagnosis encompasses emphysema and chronic bronchitis. Smoking is overwhelmingly the main driver of the condition, leading to progressive and irreversible lung destruction that severely restricts air flow, causing debilitating breathing difficulties and eventually proving fatal.
Other Respiratory Diseases: Beyond COPD, smoking worsens and contributes to the fatality of other respiratory conditions, including severe bouts of pneumonia and influenza.
Diabetes: Smoking heightens the risk of developing type 2 diabetes and makes managing the condition considerably harder, resulting in more severe complications.
Trends Over Time
Historically, the rate of smoking was much higher in many Western nations. The increase in cigarette use during the twentieth century inevitably led to an epidemic of smoking-related diseases and deaths that unfolded in the subsequent decades.
Decline in Prevalence: Over the past thirty years, many affluent nations, including the United States and the United Kingdom, have observed a marked decline in smoking prevalence. This positive change is the result of consistent public health initiatives, significant tax increases on tobacco products, widespread smoke-free regulations, and comprehensive programs to help people quit.
Lag in Mortality Decline: Although the numbers of people who smoke have fallen, the corresponding drop in smoking-related deaths often takes several decades to materialize because the diseases caused by smoking take many years to develop. Nonetheless, a positive trend is now visible: as smoking prevalence decreases, so too does the incidence of associated diseases and deaths, though the process is slow.
Global Shift: While smoking rates are receding in many economically developed nations, they remain high or are, in some cases, rising in certain low- and middle-income countries, particularly in regions of Asia and Africa. This shift means the global burden of mortality from smoking is increasingly concentrated in these areas.
Evolving Products: The proliferation of heated tobacco devices, electronic cigarettes and vaping devices, and other new tobacco products adds a layer of complexity. While they have a potential for reducing harm, their long-term health consequences are still under scrutiny, and their eventual effect on tobacco-related mortality remains unclear.
Ways to Reduce This Mortality
Lowering the mortality associated with smoking demands a unified approach that integrates individual responsibility, public health policy, and medical intervention:
Comprehensive Tobacco Control Policies:
Taxation Increases: Raising duties on tobacco products makes them prohibitively expensive, particularly for young people, and is proven to curtail consumption.
Smoke-Free Environments: Legislation banning smoking in public indoor spaces and workplaces protects non-smokers from harmful secondhand smoke and encourages smokers to reduce their intake or quit entirely.
Marketing Restrictions: Strict controls on the advertising, promotion, and sponsorship of tobacco products are crucial to prevent the recruitment of new, young users.
Plain Packaging: Standardized, simple packaging featuring large, graphic health warnings has been demonstrated to lessen the attractiveness of tobacco products.
Support for Quitting:
Access to Treatment: Ensuring broad availability of proven methods to stop smoking, including nicotine replacement therapies, prescription drugs (such as varenicline and bupropion), and tailored behavioral support, is essential.
Involvement of Healthcare Providers: Encouraging doctors, nurses, and other health professionals to routinely screen patients for tobacco use and provide brief, supportive advice along with referrals to specialized cessation services.
Public Awareness and Education:
Targeted Campaigns: Continuing to fund and implement powerful public service campaigns that clearly illustrate the specific health consequences of smoking, with a focus on reaching younger demographics.
Focus on Vulnerable Groups: Developing customized support programs for populations that exhibit higher smoking rates or face significant socio-economic disadvantages.
Replacement of cigarettes by non-combustible products:
While quitting smoking remains the fundamental measure, for some current smokers who find it difficult stop using nicotine, it is preferable to consume it from non-combustible products. Policies should facilitate this transition..
The challenge posed by smoking is not yet overcome. While considerable progress has been achieved in some parts of the world, the global death statistics serve as a powerful reminder of the lasting and potent lethality of tobacco. Sustained, strong, and innovative efforts are necessary to further diminish this preventable mortality.
Here is what you need to know about the contraceptive pill and cigarette smoking: why it is dangerous to use both together, the risks for each type of contraceptive pill, the specific risks for women of different ages, what to do to avoid these risks, and what medical supervision is needed for women who both smoke and take the pill
The Contraceptive Pill and Smoking: A Dangerous Combination You Need to Understand
If you smoke, combining the pill with cigarettes creates a significantly elevated risk to your health. This article breaks down why this combination is so dangerous, the specific risks, and what you can do to protect yourself.
Understanding the Contraceptive Pill and Its Types
The contraceptive pill comes in two main forms:
Combined Oral Contraceptives (COCs): These pills contain two hormones: estrogen and progestin. They work by preventing ovulation, thickening cervical mucus, and thinning the uterine lining. Most of the increased health risks when smoking are associated with COCs.
Progestin-Only Pills (POPs) or “Mini-Pill”: These pills contain only progestin. They primarily work by thickening cervical mucus and thinning the uterine lining, sometimes suppressing ovulation. Generally, the risks associated with smoking are significantly lower with POPs compared to COCs, but discussing any concerns with your doctor is always important.
Why is Combining COCs and Smoking So Dangerous?
The estrogen component in Combined Oral Contraceptives is the key player in this risk equation. Estrogen can increase the risk of blood clot formation. Smoking, independently, also significantly damages blood vessels and promotes clot formation.
When you combine the two, you create a “perfect storm” that drastically multiplies your risk for serious cardiovascular events:
Blood Clots (Thrombosis): Smoking causes inflammation and damage to the lining of blood vessels, making them more prone to clotting. Estrogen in COCs also makes blood more likely to clot. Together, this dramatically increases the chance of a clot forming in a vein (deep vein thrombosis, DVT) or traveling to the lungs (pulmonary embolism, PE).
Heart Attack: Both smoking and COCs increase the workload on your heart and can contribute to the narrowing of arteries. When combined, this significantly raises the risk of a heart attack, especially as you get older.
Stroke: Smoking is a major risk factor for stroke due to its effects on blood vessels and blood pressure. COCs also independently increase stroke risk. The combination is particularly dangerous, as clots can travel to the brain, or blood vessels in the brain can rupture.
Specific Risks by Age Group
The dangers of smoking while on COCs are not uniform across all ages. The risk significantly increases with age, especially for women over 35.
Under 35: While the absolute risk is lower, it is still elevated compared to non-smoking pill users. Young women who smoke and take COCs face an increased risk of DVT, PE, heart attack, and stroke.
35 and Older: For women aged 35 and above, particularly those who smoke 15 or more cigarettes per day, the risks of heart attack, stroke, and blood clots become critically high. Due to these severe risks, Combined Oral Contraceptives are generally contraindicated (not recommended and often medically prohibited) for smokers over the age of 35.
What to Do to Avoid These Risks
The message is clear: if you smoke, you should not be taking Combined Oral Contraceptives.
Quit Smoking: This is the most effective action you can take. Quitting smoking will not only reduce the risks associated with contraception but will also dramatically improve your overall health and reduce your risk for numerous other diseases, including lung cancer, heart disease, and stroke.
Seek support from smoking cessation programs, nicotine replacement therapy (NRT), or medications.
Discuss Alternatives with Your Doctor: If you cannot or choose not to quit smoking, you must explore other contraceptive methods.
Progestin-Only Pills (POPs): These are generally safer for smokers as they do not contain estrogen.
Intrauterine Devices (IUDs): Both hormonal and non-hormonal IUDs are highly effective and safe for smokers.
Contraceptive Implant (e.g., Nexplanon): A progestin-only implant that is very effective and safe for smokers.
Barrier Methods: Condoms, diaphragms, or cervical caps do not involve hormones and are safe for smokers, though less effective at preventing pregnancy compared to hormonal methods or IUDs.
Medical Supervision for Women Who Smoke and Take the Pill
If you are a smoker and currently taking a Combined Oral Contraceptive, or considering starting one, urgent medical consultation is essential.
Your doctor will:
Thoroughly assess your individual risk factors: This includes your age, smoking history (how long and how much you smoke), family history of blood clots or heart disease, blood pressure, and any other existing medical conditions.
Strongly advise cessation of smoking: They will discuss the immediate and long-term benefits of quitting and may offer resources to help you.
Recommend alternative contraception: Given the elevated risks, your doctor will likely recommend switching to a progestin-only method (like the mini-pill, implant, or hormonal IUD) or a non-hormonal method (like a copper IUD or barrier methods).
Monitor your blood pressure: Regular blood pressure checks are crucial, as both smoking and COCs can affect blood pressure, further increasing cardiovascular risk.
Never start or continue Combined Oral Contraceptives without discussing your smoking habits truthfully with your healthcare provider. Hiding your smoking status can put your life at serious risk.
Conclusion
The decision to use contraception is a personal one, but it must be an informed one. For women who smoke, especially those over 35, the risks associated with Combined Oral Contraceptives are severe and potentially life-threatening. Prioritizing your health means taking action – either by quitting smoking or by choosing a safer, non-estrogen based contraceptive method. Have an open and honest conversation with your doctor to find the best and safest path for your reproductive health.
Nicotine addiction is a loss of control over tobacco use driven by both brain changes and learned behaviors. Nicotine stimulates brain reward pathways, causing craving, withdrawal, and compulsive smoking, while routines and triggers reinforce the habit. Dependence severity can be measured with tools like the Cigarette Dependence Scale. The most effective treatment combines medications (nicotine replacement or prescription drugs) with behavioral support to address both physical cravings and psychological habits.
Definition and Symptoms
At its core, nicotine dependence is a loss of control over nicotine or tobacco use, it is a state where the body and mind have adapted to the presence of nicotine, the primary addictive chemical in tobacco. When nicotine is withheld, a cluster of uncomfortable withdrawalsymptoms emerges.
The symptoms of nicotine addiction can manifest in various ways, combining physical and psychological distress. Key indicators include:
Loss of Control: Continuing to smoke despite the awareness of serious health issues, like lung or heart disease, caused by smoking, and despite the social consequences.
Compulsive Use: Consumption despite the desire to quit. Repeated and unsuccessful attempts to quit or reduce tobacco consumption.
Social Avoidance: Giving up activities or avoiding places where smoking is prohibited because of the inability to abstain.
Withdrawal Symptoms: Experiencing symptoms upon cessation, such as intense cravings, irritability, anxiety, restlessness, difficulty concentrating, depressed mood, insomnia, increased hunger, weight gain and insomnia.
Tolerance: The disappearance of side effects (e.g. nausea) experienced by new users, a reduced effect at a given dose, and the need to consume more to alleviate cravings and withdrawal symptoms. This is especially true for new smokers, because regular smokers usually smoke the same amount over many years.
Early Morning Smoking: Lighting up a cigarette within the first 30 minutes of waking. The shorter the time to the first cigarette, the higher the degree of dependence.
Assessing the Degree of Dependence
While a clinical diagnosis of nicotine dependence is based on criteria established by psychiatric manuals, researchers and clinicians also employ self-report tests to measure its severity.
One such instrument, designed to provide a continuous and nuanced index of a smoker’s dependence, is the Cigarette Dependence Scale (CDS), developed by the author of this website and his colleagues. The shorter, 5-item version provides a quick test that can be used to tailor treatment. The longer, 12-item version (CDS-12) assessesmultiple facets of the dependence construct. By having the smoker rate statements on a five-point scale, the questionnaire provides a total score that clinicians can use to gauge the severity of the addiction, select the most appropriate treatment approach, and monitor the patient’s progress during cessation efforts.
The Biological Mechanism: Nicotine and the Brain
The invisible chain of addiction is forged in the brain’s complex circuitry. Nicotine acts as a powerful psychoactive agent, mimicking the natural neurotransmitter acetylcholine.
Upon inhalation, nicotine reaches the brain in mere seconds. There, it binds to specific protein channels, known as nicotinic acetylcholine receptors (nAChRs), located throughout the brain. When nicotine binds to these receptors, it triggers the release of several neurochemicals, most notably dopamine in the brain’s reward centers. This rush of dopamine produces the transient feelings of pleasure, focus, and reward that reinforce the act of smoking. The brain is somehow tricked to associate smoking with other rewards that are essential for survival.
With repeated exposure, the brain adapts: it produces an excess number of nAChRs in an attempt to compensate for the constant stimulation—a process called upregulation. This adaptation is the biological basis for tolerance, meaning the smoker needs more nicotine to achieve the same effect. When the nicotine supply is cut off, these upregulated receptors are left craving stimulation, leading to intense withdrawal symptoms and driving the compulsive need to smoke again. This cycle of seeking relief from discomfort is known as negative reinforcement, cementing the addiction.
The key factor is that the addictiveness of a nicotine delivery device depends on the speed at which nicotine is delivered to the blood and brain. Cigarettes have the fastest nicotine delivery, as a large amount of nicotine reaches the brain within seconds of inhaling a puff. In contrast, nicotine patches, gum, lozenges, and pouches deliver the nicotine dose much more slowly, so these products are not addictive. Electronic cigarettes and heated tobacco products have a medium delivery rate, nd some of these products can also be addictive depending on the amount and speed of nicotine delivery.
The Behavioral Component: Triggers and Rituals
Cigarette addiction is not purely chemical; it is also deeply interwoven with learned behaviors and environmental cues. This is the behavioral component of the dependence.
Smokers repeatedly link the physical act of smoking with daily routines, emotional states, and social settings. The morning coffee, the work break, driving a car, finishing a meal, talking on the phone, or experiencing stress or anxiety all become powerful cues, or “triggers,” that signal the need for a cigarette. The mere sight or smell of tobacco, or being in the presence of other smokers, can elicit a powerful craving. These ritualistic associations create a psychological dependence that must be addressed alongside the physical addiction to ensure long-term cessation.
Treatment Methods
The treatment for cigarette addiction is most effective when it is multi-faceted, addressing both the biological craving and the deeply ingrained behavioral habits, and when it combines pharmacological with behavioral treatments.
Pharmacological Treatments aim to manage the physical symptoms of withdrawal and reduce the reinforcing effects of nicotine:30
Nicotine Replacement Therapy (NRT): Available as patches, gum, lozenges, inhalers, and sprays, NRT delivers controlled doses of nicotine without the harmful toxins of tobacco smoke, and at a slower rate than cigarettes, making these products non-addictive. This helps mitigate withdrawal symptoms. Combining a long-acting form (like the patch) with a short-acting form (like the gum) for acute cravings is more effective than using either product alone.
Prescription Medications: Drugs like varenicline, cytisine and bupropion are non-nicotine options. Varenicline and cytisine work by partially stimulating the nAChR, reducing both cravings and the pleasure derived from smoking, while bupropion, originally an antidepressant, is thought to influence dopamine and norepinephrine levels to alleviate withdrawal.
Although these are not medical treatments, you can also obtain nicotine from electronic cigarettesor nicotine pouches if you do not wish to use the medications mentioned above.
Behavioral Treatments focus on disrupting the psychological and learned components of the addiction:
Cognitive Behavioral Therapy (CBT): This approach helps the smoker identify their triggers and develop effective coping strategies and relapse prevention skills. It reframes the person’s thoughts and behaviors related to smoking.
Counseling and Support: Individual or group counseling, often delivered by specialists or through telephone quitlines, provides essential support, motivation, and practical guidance on navigating the challenges of quitting.
Motivational Interviewing (MI) is a specific technique used to help ambivalent smokers explore and resolve their feelings about cessation.
Successful smoking cessation is based on a combination of medication and behavioral support tailored to your individual needs and level of dependence. Millions of people have successfully quit smoking with the help of pharmacological and behavioral aids, and you can do it too, just like them, and improve your health immediately.
Use the ‘Comments’ field below to share your experience or to suggest imporovements to this article.
References:
Etter, JF., Le Houezec, J. & Perneger, T. A Self-Administered Questionnaire to Measure Dependence on Cigarettes: The Cigarette Dependence Scale. Neuropsychopharmacol28, 359–370 (2003). https://doi.org/10.1038/sj.npp.1300030
Jean-François Etter, Comparing the validity of the Cigarette Dependence Scale and the Fagerström Test for Nicotine Dependence, Drug and Alcohol Dependence, Volume 95, Issues 1–2, 2008, Pages 152-159, ISSN 0376-8716, https://doi.org/10.1016/j.drugalcdep.2008.01.017.
Jean-François Etter, A comparison of the content-, construct- and predictive validity of the cigarette dependence scale and the Fagerström test for nicotine dependence, Drug and Alcohol Dependence, Volume 77, Issue 3, 2005, Pages 259-268, ISSN 0376-8716, https://doi.org/10.1016/j.drugalcdep.2004.08.015.