Carbon monoxide (CO) is one of the most harmful gases inhaled when smoking. It is invisible, odorless, and tasteless, yet it has immediate and significant effects on the body.
Carbon monoxide is produced whenever carbon-containing materials, such as tobacco, burn incompletely. When a cigarette is lit, it generates CO that is inhaled into the lungs and rapidly passes into the bloodstream. There, it binds strongly to hemoglobin, the molecule responsible for carrying oxygen. This binding forms carboxyhemoglobin, which reduces the blood’s capacity to transport oxygen to tissues and organs.
Each cigarette causes a measurable rise in carbon monoxide levels. After smoking a single cigarette, carboxyhemoglobin levels in the blood typically increase to around 3 to 6 percent. In people who smoke regularly, especially those consuming a pack per day, these levels often remain between 5 and 10 percent, and can be even higher in heavy smokers. By contrast, non-smokers usually have levels between 0.5 and 1 percent, meaning that smokers may carry five to ten times more carbon monoxide in their blood.
This difference is also reflected in exhaled air. In non-smokers, exhaled carbon monoxide levels are usually very low, typically around 1 to 5 parts per million (ppm). In smokers, however, exhaled CO commonly ranges from about 10 to 30 ppm, and can exceed this range depending on how recently and how heavily the person has smoked. These measurements are often used in smoking cessation programs to provide visible feedback on exposure.
Consequences:
The presence of carbon monoxide in the blood reduces oxygen delivery throughout the body, which has widespread consequences. In the short term, this leads to reduced physical performance, increased breathlessness, headaches, and a higher heart rate as the body attempts to compensate for the lack of oxygen. Over time, the strain on the cardiovascular system contributes to the development of heart disease and stroke. Carbon monoxide also damages blood vessels and accelerates the process of atherosclerosis. In individuals with existing conditions such as angina or chronic obstructive pulmonary disease, the effects can be particularly severe. In pregnant women, carbon monoxide exposure reduces oxygen supply to the fetus, increasing the risk of low birth weight and developmental complications.
How quickly does carbon monoxide disappear after quitting?
One of the most encouraging aspects of carbon monoxide exposure is how quickly the body begins to recover after smoking stops. Within about eight hours of the last cigarette, carbon monoxide levels in the blood drop by roughly half. Within 12 to 24 hours, levels return close to those seen in non-smokers. After about 48 hours, carbon monoxide is essentially eliminated from the bloodstream. As this happens, oxygen delivery improves rapidly, and many people begin to notice that breathing becomes easier and energy levels increase within a very short time.
Secondhand smoke remains one of the most underestimated health threats in modern households. Unlike the deliberate choice smokers make when lighting a cigarette, those around them—spouses, children, and guests—have no say in their exposure to toxic chemicals and carcinogens. Yet many families continue to navigate this invisible danger with little understanding of the real risks involved or how to address the problem.
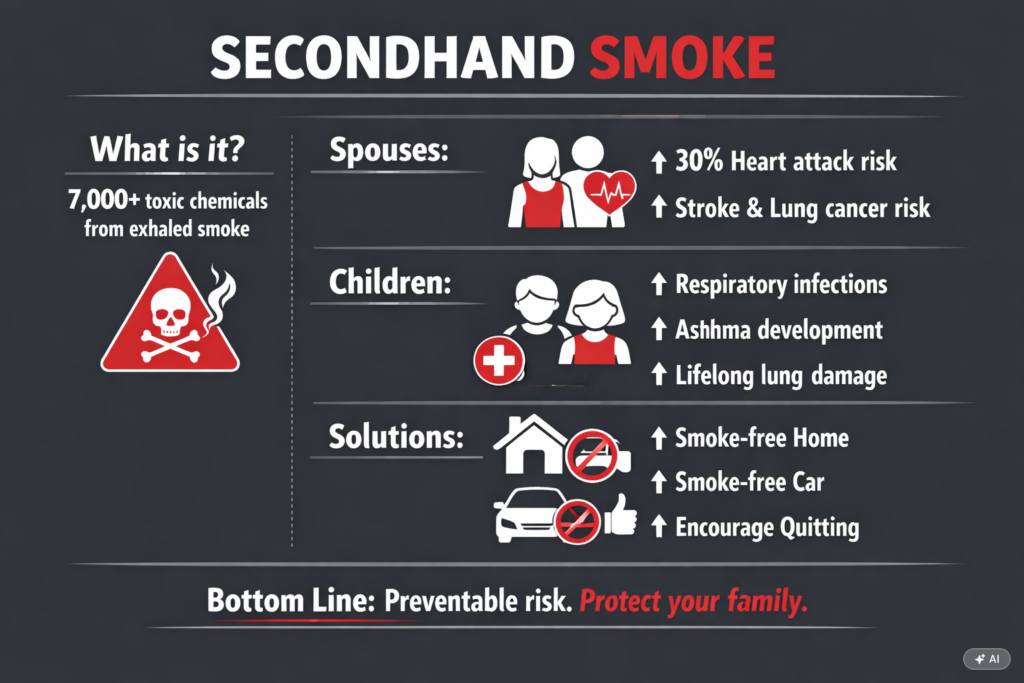
The science is clear. When a person smokes, they exhale a mixture of mainstream smoke and exhaled air, which combines with secondhand smoke to form environmental tobacco smoke, which contains more than 7,000 chemical compounds, hundreds of which are toxic and about 70 of which can cause cancer. The Environmental Protection Agency has classified secondhand smoke as a Group A carcinogen—the same category as asbestos and radon—placing it among the most dangerous substances found in homes.
Living with a smoker exposes a non-smoking spouse to the equivalent of smoking several cigarettes daily, even without ever lighting one themselves. Research consistently shows that spouses of smokers face significantly elevated risks of heart disease, stroke, and lung cancer. A study published in the journal Circulation found that non-smokers exposed to secondhand smoke at home had a 30 percent increased risk of heart attack compared to those in smoke-free homes.
The damage occurs silently and progressively. Secondhand smoke damages the lining of blood vessels, reduces oxygen in the blood, and increases the likelihood of blood clots. Over time, these effects accumulate, creating conditions for serious cardiovascular events. Women appear particularly vulnerable, with some studies suggesting even higher risks for female non-smokers in relationships with smokers.
Beyond the physical health impacts, many spouses report emotional strain. The constant exposure to smoke, despite requests to quit or smoke outside, can breed resentment and feelings of helplessness. Partners often find themselves caught between concern for their loved one’s health and frustration at being unable to protect their own.
The Particular Vulnerability of Children
Children face perhaps the most concerning risks from secondhand smoke exposure. Their lungs are still developing, their immune systems remain immature, and they spend more time in the home environment than adults. A child living with a smoker absorbs secondhand smoke continuously throughout the day and night.
The consequences are measurable and severe. Children exposed to secondhand smoke suffer higher rates of ear infections, respiratory infections, asthma development, and asthma exacerbation. They experience more coughing, wheezing, and shortness of breath. Some studies suggest that children of smokers miss more school days due to illness than their peers from smoke-free homes.
The risks extend beyond immediate respiratory concerns. Secondhand smoke exposure in childhood has been linked to reduced lung function that may persist into adulthood, even if the child is never exposed to smoke as a teenager or adult. Additionally, children living with smokers face increased risks of sudden infant death syndrome, if an infant is present, and developmental delays in some cases.
Perhaps most troubling is the modeling effect. Children who grow up in smoking households are significantly more likely to become smokers themselves, perpetuating a cycle of addiction and health consequences across generations.
Navigating Family Dynamics
Addressing smoking within a family requires sensitivity, firmness, and realistic expectations. Many people hesitate to confront a family member about smoking, fearing conflict or seeming judgmental. Yet remaining silent means accepting ongoing health risks for oneself and one’s children.
Starting a conversation requires choosing the right moment and framing the discussion around health rather than judgment or control. Rather than attacking the smoker’s choice, focus on the impact on family members. Phrases like “I’m worried about my health because of the smoke in our home” or “I want our children to grow up in a healthy environment” open dialogue without immediately triggering defensiveness.
Some families find success with compromise solutions initially. Designating smoking areas outside the home, away from doors and windows, reduces but does not eliminate secondhand smoke exposure. Improved ventilation through air purifiers can help, though no amount of ventilation completely removes secondhand smoke from indoor air. These measures work best as stepping stones toward complete smoke cessation rather than permanent solutions.
In cases where a family member refuses to quit or even reduce smoking, establishing firm boundaries becomes necessary. This might mean designating certain areas of the home as completely smoke-free, such as children’s bedrooms or the family car. It might mean limiting visits or requiring smokers to change clothes and wash hands before holding an infant. These boundaries, while sometimes difficult to enforce, communicate clearly that the health and comfort of non-smokers matter.
Practical Steps to Reduce Exposure
For those unable to convince a household member to quit immediately, several measures can minimize secondhand smoke exposure. The most effective is creating a completely smoke-free home, but when that proves impossible, establishing smoke-free zones—particularly children’s bedrooms and sleeping areas—provides some protection during vulnerable hours.
Ventilation helps but has limits. Opening windows or using exhaust fans removes some smoke but cannot eliminate it entirely, particularly in smaller spaces or during cold weather when windows remain closed. Air purifiers equipped with HEPA and activated charcoal filters capture some particles and odors but cannot filter out all gaseous components of secondhand smoke.
In vehicles, the situation is even more critical. A single cigarette smoked in a car exposes passengers to secondhand smoke concentrations far exceeding those found in homes, even with windows open. Many families find that establishing a strict no-smoking policy in the car becomes a crucial boundary for protecting children during transit.
Regular cleaning can reduce the accumulation of thirdhand smoke—the toxic residue that settles on surfaces and can be reactivated into the air. Washing bedding frequently, vacuuming with HEPA filters, and wiping down surfaces where smoke settles helps somewhat, though this approach addresses symptoms rather than the underlying problem.
Solutions
For those seeking to reduce their exposure, the most effective long-term strategy remains encouraging the smoker to quit. Resources exist, from nicotine replacement therapies to counseling services to support groups. Framing smoking cessation not as giving up something valued but as gaining health, freedom, and the ability to protect loved ones can sometimes shift perspective.
Until that happens, families must take whatever protective measures they can while continuing to advocate for complete smoke cessation. No child should grow up breathing secondhand smoke. No spouse should accept health risks to avoid conflict. The conversation may be difficult, but the alternative—silent, ongoing harm to those we love—is far worse.
Use the ‘Comments’ field below to share your experience or to suggest improvements to this page.
When a cigarette burns, the combustion process acts like a mini chemical factory, creating toxic substances that are not present in unburned tobacco and releasing a cloud of smoke containing thousands of compounds, many of which are highly toxic, carcinogenic, or pharmacologically active. Smoke is the real disease vector, attacking virtually every system in the body with each inhalation. Understanding the types of substances present and how manufacturers design them is essential to grasping the health risks of smoking.
The Three Classes of Toxic Agents
Cigarette smoke is typically analyzed by dividing its components into two main phases: the particulate phase (tiny solid particles and liquid droplets) and the gas phase. Within these phases, the toxic substances fall into three broad categories:
Carcinogens (Cancer-Causing Agents): These are perhaps the most feared components. Cigarette smoke contains at least 70 known human carcinogens. These chemicals damage DNA, the blueprint of the cell, leading to uncontrolled growth and tumor formation. Prominent examples include:
Polycyclic Aromatic Hydrocarbons (PAHs): Found in coal tar and automobile exhaust, PAHs are potent DNA damagers.
Nitrosamines (NNN and NNK): These are tobacco-specific carcinogens formed during the curing and burning of the tobacco leaf.
Aromatic Amines (e.g., 4-aminobiphenyl): Linked strongly to bladder cancer, these compounds are highly toxic even at low concentrations.
Pharmacologically Active and Addictive Agents: The most dominant of these is nicotine, but other substances modulate its effect and overall toxicity.
Nicotine: The primary addictive agent. While not a major cause of cancer itself, nicotine acts on the brain to drive dependence. It elevates heart rate and blood pressure, placing significant stress on the cardiovascular system.
Monoamine Oxidase (MAO) Inhibitors: As discussed previously, these compounds found in smoke artificially boost mood-regulating chemicals like dopamine in the brain, enhancing the addictive power of nicotine and making withdrawal more difficult.
Toxic and Respiratory Irritants: These compounds damage the airways and interfere with the body’s ability to use oxygen.
Carbon Monoxide (CO): A colorless, odorless, deadly gas. CO is inhaled and quickly binds to hemoglobin in the blood, displacing oxygen. This reduces the oxygen-carrying capacity of the blood, starving organs, including the heart and brain, of necessary oxygen. This oxygen deprivation, known as hypoxia, is a major contributor to cardiovascular disease in smokers.
Hydrogen Cyanide: A chemical warfare agent, this gas impairs the lungs’ natural cleaning system—the cilia—making it harder for the lungs to clear mucus and foreign particles, thereby increasing the risk of infection and chronic inflammation.
Acrolein and Ammonia: Both are highly irritating gases that damage the delicate lining of the airways and alveoli, directly contributing to the inflammation and destruction seen in Chronic Obstructive Pulmonary Disease (COPD).
How Manufacturers Engineer Nicotine Dosage
The tobacco industry employs highly precise engineering to ensure the maximum, addictive delivery of nicotine, often with the same chemical rigor used in pharmaceutical manufacturing. This control is achieved through three main levers:
Ammonia Technology: By treating tobacco with ammonia or its compounds, manufacturers increase the alkalinity (pH) of the smoke. This process converts the bound nicotine in the tobacco into its “freebase” form. Freebase nicotine is vaporized more easily and absorbed into the bloodstream far more quickly and intensely, producing a rapid, powerful “hit” that maximizes the addictive potential of the product.
Filter and Ventilation Control: As discussed previously, while filters outwardly suggest reduced harm, the tiny ventilation holes laser-perforated into the filter paper are designed to game machine testing. They dilute the smoke when measured, allowing “low-tar” claims. In real-world use, however, smokers instinctively cover these holes or inhale more deeply to get their required dose of nicotine, effectively bypassing the filter’s diluting function. This engineering ensures that the intended addictive dose is always met.
Controlling the Smell (Odor) of Secondhand Smoke
The perception of cigarette smoke—the harshness and the lingering odor—is a factor that can deter non-smokers and affect social tolerance of the product. Manufacturers have, over time, used additives not just to improve the taste for the user, but to modify the odor of the side-stream smoke (the smoke coming directly from the burning tip).
Flavorings and aromatic compounds are included to create a more “pleasant” aroma, making the smoke less irritating to bystanders and potentially reducing the social stigma associated with smoking in certain environments. This chemical masking is a strategic move to maintain social acceptance and increase the perceived appeal of the product, despite the unchanged underlying toxicity of the thousands of chemicals in the aerosol.
The cigarette, therefore, is not a simple natural product. It is a highly engineered, chemically saturated delivery system designed to addict the user and facilitate the transport of hundreds of poisons directly into the body, a process that is precisely controlled from the tobacco field to the filter tip.
Many people know that nicotine makes cigarettes addictive, but few know how much nicotine is actually in a cigarette, or how much nicotine your body absorbs when you smoke. Understanding these numbers can help you choose an alternative product that does not involve burning tobacco or inhaling smoke.
How much nicotine is in a cigarette?
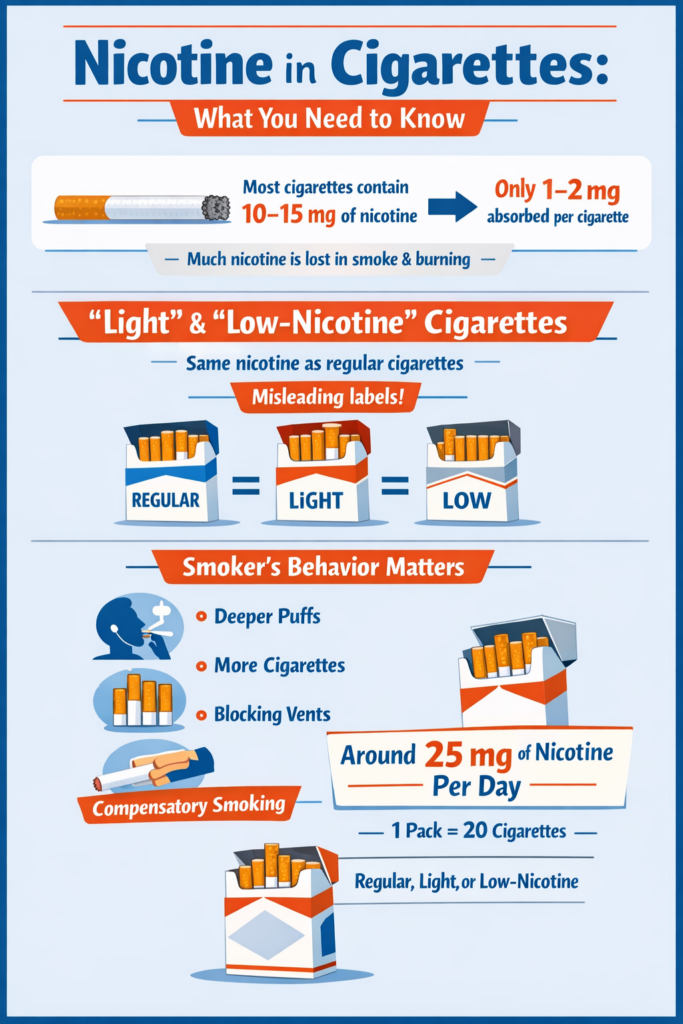
The total amount of nicotine in a cigarette varies, but most commercial cigarettes contain between 10 and 15 milligrams (mg) of nicotine. This is the amount present in the tobacco before the cigarette is lit, but this figure does not reflect the whole picture. Most of the nicotine in a cigarette is destroyed by combustion or remains in the sidestream smoke that you do not inhale. What really matters is the amount of nicotine that enters your bloodstream.
‘Light’ or ‘low-nicotine’ cigarettes:
Don’t be fooled by these labels! Studies have shown that cigarettes marketed as ‘light’ or ‘low-nicotine’ contain about the same amount of nicotine as regular cigarettes. The real difference lies in their design (air holes around the filter), which can affect how you smoke.
How much nicotine do you actually inhale?
You do not inhale all of the 10 to 15 mg of nicotine contained in a cigarette. When you light a cigarette and take a puff, a significant amount of nicotine is destroyed by heat or escapes as sidestream smoke. The amount of nicotine that enters your lungs and is absorbed in your blood (bioavailability) depends on many factors, including how the cigarette is manufactured and, most importantly, how you smoke it. A person who smokes one cigarette absorbs approximately 1 to 2 mg of nicotine. Although this amount may seem small compared to the total 15 mg, it is enough to deliver a powerful dose to your brain and satisfy your addiction.
The smoker’s behavior matters
The way a person smokes is the most important variable in the actual dose received. Each person behaves differently, and two people smoking the same cigarette may absorb different amounts of nicotine. Your brain acts like a thermostat that determines how much nicotine you need to feel good and avoid nicotine withdrawal symptoms. As a result, people who smoke “low nicotine” or “light” cigarettes do so differently than normal cigarettes. This is called compensatory smoking:
Deeper puffs: If you use a low-nicotine cigarette, your body compensates by taking deeper, longer puffs to get the amount of nicotine your brain needs.
Smoking more often: You may also simply smoke more cigarettes throughout the day.
Blocking the vents: Some ‘light’ cigarettes have ventilation holes near the filter. Smokers often cover these with their fingers or lips, either unconsciously or intentionally, which increases the concentration of smoke inhaled and, consequently, the dose of nicotine.
This means that a heavy smoker can easily absorb 25 mg of nicotine per day by smoking a pack of 20 cigarettes, whether these are regular, low-nicotine or light cigarettes.
Why it is important to understand nicotine levels and the speed of delivery:
Nicotine is the main addictive chemical in tobacco, it is what drives you to smoke one cigarette after another. When you inhale smoke, nicotine quickly enters your bloodstream and reaches your brain. This rush causes the release of a chemical that makes you feel good (dopamine), which is why smoking can be enjoyable or soothing. But this feeling is temporary, as the nicotine level in your blood drops quickly, leading to withdrawal symptoms.
When you smoke, nicotine reaches your brain within 10 to 20 seconds of inhalation. This rapid effect is one of the reasons why cigarettes are so addictive. Your brain learns to anticipate this rapid rush, and cravings develop when nicotine levels drop. Nicotine replacement therapies (patches, gum, tablets) release nicotine at a much slower rate and therefore do not create addiction, even though the molecule is the same.
Understanding how nicotine works helps to understand why nicotine replacement therapies (such as patches, gum or lozenges) are designed in this way: to provide controlled, lower doses of nicotine at a slower rate of delivery and without the toxic chemicals found in cigarette smoke.
Knowing all this can make it easier to quit smoking.
Knowing these figures can help you understand how cigarettes are designed to make you addicted. The tobacco industry adjusts the chemical composition so that nicotine reaches your brain quickly and reliably, not only by controlling the amount of nicotine in cigarettes with the same precision used by drug manufacturers to produce prescription drugs, but also by using chemical additives.
To quit smoking without experiencing nicotine withdrawal symptoms, you need to replace the “dirty” nicotine you currently get from smoking with “clean” nicotine from nicotine replacement therapy (NRT): products such as patches, gum and lozenges deliver a controlled and steady dose of nicotine without the thousands of other toxic chemicals found in cigarette smoke. Nicotine-based medicines release nicotine at a much slower rate than cigarettes, which is why these products are not addictive. They help you manage withdrawal symptoms when you quit smoking.
Behavioural support from a healthcare professional increases the effectiveness of nicotine replacement therapy. Peer support groups and quit-smoking helplines can also help you manage the psychological and behavioral aspects of quitting smoking.
If you do not want to use NRT, you can also get nicotine from e-cigarettes or nicotine pouches, these products deliver sufficient amounts of nicotine but no smoke, and are therefore much less dangerous than cigarettes.
Rate this article by clicking on the desired number of stars: (1 votes, average: 5.00 out of 5) Loading...
Please use the “Comments” field below to share your experience or suggest improvements to this article.