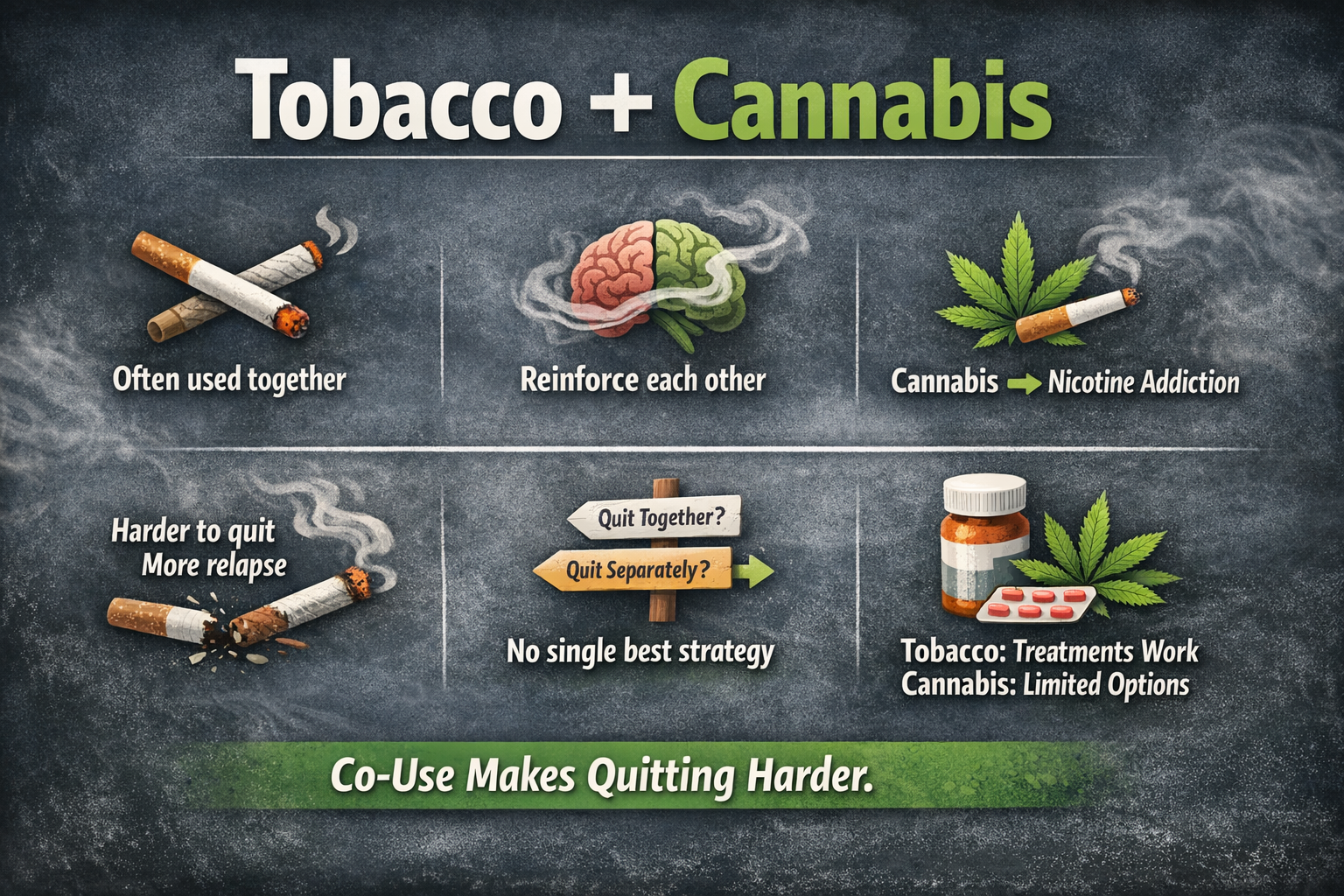
The article explains how tobacco and cannabis reinforce each other biologically and behaviorally. While THC and nicotine target distinct but interacting systems in the brain, cannabis often acts as a gateway that leads to or sustains nicotine addiction. Because cannabis use is a major trigger for tobacco relapse, experts generally recommend quitting both simultaneously to break the cycle. While specific medications for cannabis are limited, combining traditional nicotine replacement therapy with behavioral support offers the best chance at a clean break.
A shared landscape of use
Globally, tobacco remains one of the most widely consumed psychoactive substances, with more than a billion users. Cannabis, once more marginal, now counts nearly 200 million users worldwide. What is striking is not only the scale of each phenomenon, but their intersection. Among people who use tobacco, cannabis use is disproportionately common, and vice versa. In some populations, more than half of cannabis users also smoke tobacco (1).
This overlap is not incidental. In countries where both substances are widely available, roughly one in three tobacco users also consumes cannabis (2), and daily cannabis use is markedly higher among smokers than among non-smokers (3). Among young users of nicotine products, co-use rates can exceed 50% (4). What emerges is not two parallel epidemics, but a shared behavioral ecosystem.
Why people use both
The reasons for co-use are as much cultural as they are pharmacological. For some, tobacco enhances the psychoactive effects of cannabis; for others, cannabis softens the stimulation of nicotine. Mixing the two is common practice in many regions.
But beyond habit and ritual lies a deeper interaction. Users report that one substance can trigger cravings for the other, or serve as a substitute when the preferred drug is unavailable. This behavioral coupling reflects overlapping reward pathways in the brain, where both nicotine and THC act on interconnected neurochemical systems.
Social context also plays a decisive role. Initiation often occurs in shared environments—peer groups, nightlife, or informal settings—where the boundary between substances is blurred. Over time, this proximity fosters conditioning: the act of smoking, regardless of the substance, becomes a cue in itself.
From cannabis use to nicotine dependence
One of the most underappreciated pathways in addiction is the role cannabis can play in initiating or reinforcing nicotine dependence. This occurs through several mechanisms.
First, co-administration—mixing tobacco with cannabis—introduces nicotine to individuals who might not otherwise use tobacco. This is particularly evident when cannabis is consumed with tobacco rather than in pure form.
Second, repeated exposure to nicotine, even at low doses, can lead to dependence. Evidence suggests that cannabis users who also smoke tobacco exhibit higher levels of nicotine dependence than those who smoke cigarettes alone.
Third, the relationship is bidirectional. Tobacco use appears to increase the risk of cannabis dependence and relapse, while cannabis use increases the likelihood of developing nicotine dependence and makes quitting tobacco more difficult.
In short, cannabis does not merely coexist with tobacco; it can act as a gateway into sustained nicotine addiction.
Nicotine, THC, and the brain
Nicotine and THC operate through distinct but interacting systems in the brain. Nicotine stimulates nicotinic acetylcholine receptors, leading to the release of dopamine in reward circuits. THC, the main psychoactive compound in cannabis, acts primarily on the endocannabinoid system, modulating neurotransmitter release and influencing mood, memory, and perception.
Where it becomes complex is in their interaction. Experimental and clinical studies suggest that nicotine may partially offset some cognitive impairments associated with cannabis use, particularly in memory (5). This “compensatory” effect may reinforce co-use: users perceive a functional benefit in combining the two.
At the same time, the endocannabinoid system appears to play a role in nicotine dependence itself, influencing craving and withdrawal. The two substances are not simply additive; they are biologically intertwined.
Quitting tobacco in the context of cannabis use
One of the most challenging realities is that cannabis use complicates smoking cessation. People who use both substances tend to experience more intense withdrawal symptoms during tobacco quit attempts, at least in the early stages (6).
Relapse is also more common. Cannabis can act as a trigger—both behaviorally and neurochemically—reactivating the urge to smoke tobacco. Conversely, quitting tobacco may lead some individuals to increase cannabis use as a form of compensation, a phenomenon observed in several studies.
The evidence is not entirely consistent, but the overall picture is clear: co-use introduces instability into the quitting process.
Quit together or separately?
This question has no universal answer, and the scientific literature reflects that ambiguity. Some data suggest that addressing both substances simultaneously may prevent substitution effects and improve overall outcomes. Others indicate that focusing on one substance at a time may be more manageable for certain individuals.
What is increasingly recognized is that co-users are not a homogeneous group (7). Patterns of use vary—simultaneous versus separate, daily versus occasional, dependent versus recreational—and these differences matter. Tailored approaches, rather than one-size-fits-all strategies, are likely to be more effective.
Treatment options: what works, what doesn’t
For tobacco cessation, the evidence base is strong. Nicotine replacement therapies, varenicline, cytisine and bupropion remain the cornerstone treatments, combined with behavioral support.
For cannabis, the situation is more uncertain. No pharmacological treatment has yet demonstrated consistent efficacy for cannabis use disorder. Behavioral interventions—cognitive-behavioral therapy, motivational interviewing, contingency management—remain the primary tools.
For people who use both substances, integrated treatment approaches are still rare. Clinical trials have only begun to address co-use directly, and the results are modest. Interventions may reduce cannabis consumption, but their impact on tobacco cessation is less clear (8).
This gap reflects a broader issue: healthcare systems are still largely organized around single-substance models, while real-world use is increasingly multi-substance.
Use the ‘Comments’ field below to share your experience and to suggest improvements to this article, or write a testimonial.