You often hear about daily smokers, but what about those who only smoke occasionally—maybe a cigarette on the weekend, a few times a month, or even just during a yearly vacation? If you’re a former smoker who sometimes considers “just one puff,” or if you currently identify as a non-daily or occasional smoker, this article is for you.
🤔 Not All Smokers Are Addicted
It’s true that not every person who smokes is addicted to nicotine. While many non-daily smokers do have some level of dependence, others smoke primarily due to habit, social cues, or psychological triggers (like stress or boredom) without experiencing severe withdrawal symptoms when they stop.
Occasional Smokers: These individuals might smoke a few times a month or a year. Their behavior is often tied to specific social situations (e.g., parties, bars) or emotional states.1 They may not feel a strong physical need for nicotine.
Non-Daily Smokers: These individuals smoke, but not every day. They might smoke a few cigarettes on the weekend but none during the week. This pattern is often the grey area where dependence is developing or already present, but perhaps not as intense as in a daily smoker.
However, regardless of the level of addiction, any level of smoking carries risks.
🚨 The Surprising Health Risks of Occasional Smoking
The idea that “just a few” cigarettes can’t hurt is a dangerous myth. Research shows that non-daily and occasional smoking poses significant health risks.
Heart Disease: Occasional smoking significantly increases the risk of heart disease, almost doubling it compared to non-smokers. Even small amounts of smoke can damage blood vessels and increase the risk of blood clots.
Lung Cancer: While the risk is lower than for heavy smokers, occasional smokers are still several times more likely to develop lung cancer than people who have never smoked. There is no truly “safe” threshold for cigarette smoke exposure.
Other Cancers: Occasional smoking increases the risk of other cancers, including those of the esophagus, stomach, and bladder.
Respiratory Issues: Even occasional smoking can impair lung function and increase the risk of respiratory infections.
The takeaway? When it comes to the toxic substances in tobacco smoke, your body suffers damage with every puff, although the risk increases with the number of cigarettes smoked per day, the frequency, and the duration of smoking.
🔙 The High Risk of Relapse for Former Smokers
If you have already quit smoking, the biggest threat is the thought that you can handle “just one” cigarette or “just a puff.”
Nicotine’s Power: Nicotine is highly effective at re-awakening the dormant addiction pathways in your brain. A single puff is often enough to remind your brain of the “reward” it used to receive.
The “Slippery Slope”: That single puff can easily lead to one cigarette the next week, then two the week after, and soon you find yourself back to daily smoking. Relapse rarely happens overnight; it starts with an occasional exception.
The Re-Establishment of Triggers: Even an occasional cigarette re-establishes the psychological connection between smoking and your daily life (stress, coffee, alcohol). This makes future cravings much stronger and harder to manage.
✋ Your Golden Rule: Not Even a Single Puff
For anyone serious about staying quit, the most important rule is the simplest: You must never take another puff of tobacco.
This strict policy is your strongest defense against relapse. It eliminates the need for decision-making in a weak moment: the answer is always no.
If you are currently an occasional smoker who wants to stop before a full addiction takes hold, or a former smoker fighting the urge to try just one, remember: There is no healthy or safe level of smoking.
Rate this article by clicking on the desired number of stars: (1 votes, average: 1.00 out of 5) Loading...
Please use the “Comments” field below to share your experience or suggest improvements to this article.
Nicotinic receptors in the brain, hungry for their nicotine meal
Craving, the irresistible and uncontrollable urge to light a cigarette is a major obstacle when trying to quit smoking. Understanding what a craving is, where it comes from, and how to deal with it is essential to successfully quitting smoking.
What is a Craving and What Causes It?
Simply put, a smoking craving is a powerful physical and psychological impulse to smoke or to use nicotine immediately.
The Root Cause: Nicotine Addiction
The core of the craving is your brain’s dependence on nicotine. When it is inhaled in tobacco smoke, nicotine is highly addictive (but the same nicotine in a nicotine patch is not addictive at all), and it alters the chemistry and the structure of your brain. Over time, your brain adapts: the number of nicotinic receptors increases and you start to need nicotine to feel “normal.” When you quit smoking, the nicotine level in your blood drops, and your brain sends out a distress signal, which we experience as a craving.
The Triggers: Conditioning and Habit
Smoking is heavily linked to daily routines and emotional states.5 Your brain has been conditioned to associate certain activities or feelings with smoking.6 These triggers fall into several categories:
Routine: Coffee, after a meal, driving, taking a break.7
Emotional: Stress, boredom, feeling happy or sad.8
Social: Being with friends who smoke, having a drink.9
Environmental: A specific armchair, a smoking spot outside work where you used to smoke.
The 5-Minute Rule: a Powerful Tool
Here’s the single most important fact to remember about a craving: It’s intense, but it’s short-lived.
Research shows that the strongest part of a craving usually peaks and disappears after about five minutes.10
Your job isn’t to make the craving vanish instantly; it’s to ride the wave for those few minutes until it naturally subsides. Remind yourself: “I just need to make it through the next five minutes.”
The Role of Nicotine Replacement and Other Aids
Don’t feel you have to fight this battle on willpower alone. Nicotine Replacement Therapy (NRT) and other aids are designed to give your brain the small, clean dose of nicotine it craves, without the thousands of toxins in cigarette smoke, helping you manage withdrawal symptoms.13
Nicotine Replacement Therapy (NRT): Patches provide a steady background dose, while gums, lozenges, inhalers, or sprays are “quick-response” aids you can use immediately when a craving strikes.14 They are excellent for helping you get past that critical 5-minute peak.
E-Cigarettes (Vaping): Vaping can serve as a transition tool.15 It mimics the hand-to-mouth action and provides nicotine in good flavors.
Oral Tobacco (Snus/Nicotine Pouches): These are sometimes used for harm reduction in places where they are legally available, offering a smoke-free nicotine source.16
How to Deal with the Urge: Distraction is Key
Since the urge is temporary, your strategy is simple: Distract yourself until the five minutes pass. You need quick, engaging activities that interrupt the thought process.
Distraction Techniques
Move Your Body: Get up and walk around the house or office. Do 10 quick squats or push-ups.
Engage Your Hands: Play a quick game on your phone, doodle, chew gum, sip water slowly, or crunch on a carrot stick.11
Change Your Scenery: Step outside for a breath of fresh air (away from smoking areas), or move to a different room.12
Focus on Your Breath: Take five slow, deep breaths, counting to four on the inhale and four on the exhale.
Talk it Out: Send a text to a friend, or call a quitting support line.
Specific Triggers and How to Control Them
Triggers require a pre-planned response. Think of them as battle zones where you need a prepared counter-strategy.
If the Urge Strikes…
Try This Action Plan
When you wake up
Don’t leave the bedroom immediately. Drink a large glass of water, do a 2-minute stretch, chew a piece of nicotine gum, or brush your teeth.
After a meal
Replace the ritual. Immediately get up and clean the dishes, brush your teeth, chew a piece of nicotine gum, or call a friend for a quick chat.
In the presence of smokers
Distance yourself. Announce, “I’m going to grab a drink/fresh air,” and walk away for 5-10 minutes until they’ve finished their cigarette. Chew a piece of nicotine gum.
In a stressful situation
Focus on breathing. Use deep-breathing exercises. Take a 5-minute time-out to write down what’s stressing you, then crumple the paper.
In a place you used to smoke
Change the environment. Sit in a different chair, or physically block the usual smoking area (e.g., place a flowerpot there) to break the association.
Every time you beat a craving, you weaken the addiction and strengthen your resolve. You are retraining your brain, one five-minute victory at a time. Keep going !
Rate this article by clicking on the desired number of stars: (1 votes, average: 5.00 out of 5) Loading...
Please use the “Comments” field below to share your experience or suggest improvements to this article.
Our previous research found that a value of 16 or above indicates that your are strongly addicted to cigarettes.(a)
This questionnaire is called the Cigarette Dependence Scale (CDS-5), it is a well-validated measure of dependence.(b)
References:
a) Etter JF, Comparing the validity of the Cigarette Dependence Scale and the Fagerström Test for Nicotine Dependence, Drug and Alcohol Dependence, Volume 95, Issues 1–2, 2008, Pages 152-159, ISSN 0376-8716, https://doi.org/10.1016/j.drugalcdep.2008.01.017.
b) Etter, JF., Le Houezec, J. & Perneger, T. A Self-Administered Questionnaire to Measure Dependence on Cigarettes: The Cigarette Dependence Scale. Neuropsychopharmacology 28, 359–370 (2003). https://doi.org/10.1038/sj.npp.1300030
Please rate this article by clicking on the desired number of stars: (2 votes, average: 5.00 out of 5) Loading...
Please use the “Comments” field below to share your experience or suggest improvements to this article.
Answer these 5 questions to assess your nicotine consumption as a smoker (or your consumption when you smoked). We will then use this information to calculate the optimal nicotine concentration in your e-liquids, nicotine-based medications (patches, gum, tablets, inhalers), or nicotine pouches. Our statistics show that these 5 questions allow us to estimate your nicotine needs with twice the accuracy of using only the number of cigarettes smoked per day.
1- How many cigarettes do (did) you usually smoke per day?
1-5 cig./day = 1 point
6-10 cig./day = 2 points
11-15 cig./day= 3 points
16-20 cig./day= 4 points
21+ cig./day = 5 points
2- Usually, how long after waking up do (did) you smoke your first cigarette of the day?
0-5 minutes = 5 points
6-15 minutes = 4 points
16-30 minutes = 3 points
31-60 minutes = 2 points
Over 1 hour = 1 point
3- On a scale of 0 to 100, indicate how heavily you smoke(d):
0 = 0 point
1-20 = 1 point
21-40 = 2 points
41-60 = 3 points
61-80 = 4 points
81-100 = 5 points
4- On a scale of 0 to 10, how much smoke do you inhale each day (or inhaled when you smoked)? This amount depends on the number of cigarettes you smoke, how deeply you inhale, and the number of puffs. 0: I do not inhale any smoke. 10: I smoke so much that even if I tried, I couldnot inhale any more smoke.
0 = 0 point
1-2 = 1 point
3-4 = 2 points
5-6 = 3 points
7-8 = 4 points
9-10 = 5 points
5- Indicate the number of milligrams of nicotine listed on your cigarette packet:
0.1-0.5 mg = 1 point
0.6-0.7 mg = 2 points
0.8 mg = 3 points
0.9 mg = 4 points
1.0 mg or more = 5 points
Now, add up and calculate your total number of points (maximum = 25 points)
Data from our studies indicate that if your total is:
0-4 points, you aborb between 0 and 7 mg of nicotine per day (mean = 3.4 mg / day)
5-9 points, you aborb between 7 and 14 mg of nicotine per day (mean = 10 mg / day)
10-14 points, you aborb between 14 and 21 mg of nicotine per day (mean = 17 mg / day)
15-19 points, you aborb between 21 and 28 mg of nicotine per day (mean = 24 mg / day)
20-25 points, you aborb over 30 mg of nicotine per day.
After quitting smoking, you must continue to absorb the same amount of nicotine in order to avoid withdrawal symptoms and to prevent yourself from starting smoking again because you cannot tolerate these symptoms. Consume enough nicotine from e-cigarettes, nicotine-based medications, or nicotine pouches for at least 3 months after quitting smoking.
Dosage for nicotine medications
Nicotine replacement medications release approximately 70% of the nicotine they contain. For example, a patch containing 21 mg of nicotine releases approximately 15 mg of nicotine.
Use this factor (x 0.7) to calculate the optimal dose of your nicotine medication. For example, if you scored 12 points on our questionnaire, you need 17 mg of nicotine per day, and a 21 mg patch plus two 2 mg gums should provide you with the necessary dose.
Dosage for nicotine pouches
Use the same rule (x 0.7) as for nicotine medications.
Dosage for e-cigarettes
For e-cigarettes, the amount of nicotine aborbed by the user depends on many factors, in addition to the nicotine concentration in the e-liquid:
the other characteristics of the e-liquid (flavor, nicotine salt or freebase nicotine),
the characteristics of the device (battery, coil, wick)
your own level of nicotine addiction, your personal way on inhaling (number and depth of puffs), your social environment (whereas you are around smokers and vapers).
Nevertheless, our previous studies conducted among former smokers who successfully quit smoking using e-cigarettes, and who responded to the above questionnaire offer some insights.
Vapers who were ex-smokers and obtained :
0-4 points used e-liquids containing 10 mg / mL
5-9 points used e-liquids containing 10-12 mg / mL
10-14 points used e-liquids containing 12 mg / mL
15-19 points used e-liquids containing 16 mg / mL
20-25 points used e-liquids containing 18 mg / mL
Use these results as a guide to choose your e-liquid, and do not underdose your e-liquids, because if you do, you risk unnecessarily:
using too much liquid,
exposing your lungs to too much vapour,
spending too much money on e-liquids,
experiencing nicotine withdrawal symptoms and running the risk of relapsing into smoking.
Remember: the right dose of nicotine is the one that eliminates nicotine withdrawal symptoms. Your brain acts like a thermostat, regulating the amount of nicotine you need. If you use e-liquids that do not contain enough nicotine, you will need more liquid to feel satisfied.
There is no risk of nicotine overdose in regular smokers, as they can tell when they are consuming too much nicotine (specific taste in the mouth, sensation similar to that felt when you have smoked too much).
4 important points to remember
To successfully quit smoking and avoid nicotine withdrawal symptoms, you need a sufficient amount of nicotine. Do not underdose your nicotine products.
You need a sufficient concentration of nicotine in your e-liquids (at least 10 mg/mL). Do not listen to retailers who insist that you buy 3 mg/mL liquids, they do this because they want to sell you more liquid.
Purchase your electronic cigarettes and e-liquids from a specialist shop rather than a kiosk or online, as the sales staff in these shops can advise you and allow you to try and taste different products until you find the one that best suits your needs.
The advice provided here does not replace that of a doctor or psychologist specialising in the treatment of nicotine addiction.
Rate this article by clicking on the desired number of stars: (2 votes, average: 5.00 out of 5) Loading...
Please use the “Comments” field below to share your experience or suggest improvements to this article.
Quitting smoking causes nicotine withdrawal: cravings, mood changes (irritability, sadness, anxiety), sleep problems, difficulty concentrating, increased appetite and weight gain. Withdrawal symptoms can be eased with nicotine replacement therapies or other non-combustible nicotine sources.
What happens when you stop smoking?
When you stop smoking, your body no longer gets its dose of nicotine, and it’s normal to feel uncomfortable. Here are the withdrawal symptoms you may experience:
A very strong urge to smoke (craving)
Being in a bad mood : – sad or depressed, – angry, irritated, – impatient or agitated.
Anxious or nervous, rapid mood swings.
Poor sleep (insomnia).
Difficulty concentrating.
Increased hunger and weight gain.
But quitting smoking also brings about a rapid improvement in smell and taste.
How long does it last?
These symptoms are most intense during the first few hours and days after your last cigarette. After the first few days, these feelings diminish significantly, but be aware that some signs may last longer. The urge to smoke may return at times for several months. This is normal, but it will pass. Some people feel sad or depressed for a long time. Talk to your doctor if this is the case for you. Weight gain may be permanent.
What can you do ?
To attenuate these withdrawal symptoms, you can use nicotine medications (patch, gum, tablet, inhaler). You can also use another nicotine source that does not burn tobacco, such as an e-cigarette or a nicotine pouch. Cravings last just a few minutes, so just wait 5 minutes and it will pass
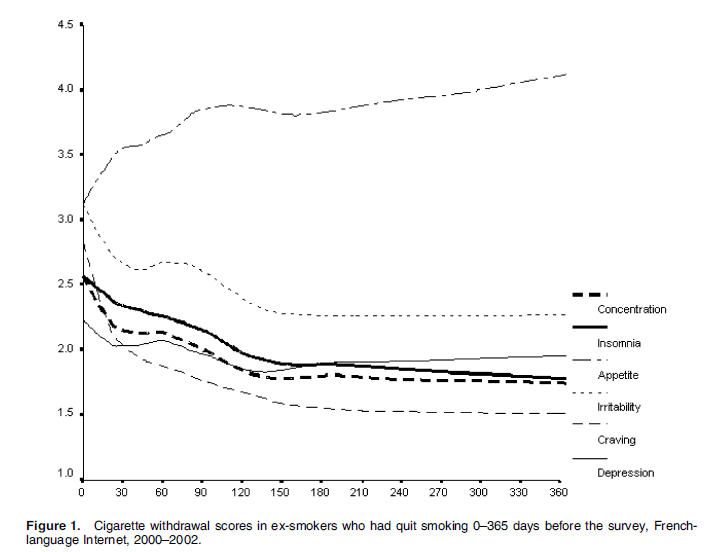
Change in symptom intensity over the course of a year
The graph below, taken from one of the author’s scientific publications, shows how the intensity of withdrawal symptoms changes during the first year after quitting smoking. The most striking feature is that appetite and weight gain increase, while the intensity of all other symptoms decreases over time. The symptom that decreases most rapidly in intensity is craving, i.e. the strong urge to smoke. The intensity of all symptoms changes most rapidly during the first 30 days after quitting smoking. AFter about 6 months, symptoms remain stable.
References:
Jean-François Etter, A Self-Administered Questionnaire to Measure Cigarette Withdrawal Symptoms: The Cigarette Withdrawal Scale, Nicotine & Tobacco Research, Volume 7, Issue 1, February 2005, Pages 47–57, https://doi.org/10.1080/14622200412331328501
Etter JF, Hughes J. A comparison of the psychometric properties of three cigarette withdrawal scales. Addiction, 2006,101,262-372.
Please rate this article by clicking on the desired number of stars: (1 votes, average: 5.00 out of 5) Loading...
Please use the “Comments” field below to share your experience or suggest improvements to this article.
Nicotine addiction is a loss of control over tobacco use driven by both brain changes and learned behaviors. Nicotine stimulates brain reward pathways, causing craving, withdrawal, and compulsive smoking, while routines and triggers reinforce the habit. Dependence severity can be measured with tools like the Cigarette Dependence Scale. The most effective treatment combines medications (nicotine replacement or prescription drugs) with behavioral support to address both physical cravings and psychological habits.
Definition and Symptoms
At its core, nicotine dependence is a loss of control over nicotine or tobacco use, it is a state where the body and mind have adapted to the presence of nicotine, the primary addictive chemical in tobacco. When nicotine is withheld, a cluster of uncomfortable withdrawalsymptoms emerges.
The symptoms of nicotine addiction can manifest in various ways, combining physical and psychological distress. Key indicators include:
Loss of Control: Continuing to smoke despite the awareness of serious health issues, like lung or heart disease, caused by smoking, and despite the social consequences.
Compulsive Use: Consumption despite the desire to quit. Repeated and unsuccessful attempts to quit or reduce tobacco consumption.
Social Avoidance: Giving up activities or avoiding places where smoking is prohibited because of the inability to abstain.
Withdrawal Symptoms: Experiencing symptoms upon cessation, such as intense cravings, irritability, anxiety, restlessness, difficulty concentrating, depressed mood, insomnia, increased hunger, weight gain and insomnia.
Tolerance: The disappearance of side effects (e.g. nausea) experienced by new users, a reduced effect at a given dose, and the need to consume more to alleviate cravings and withdrawal symptoms. This is especially true for new smokers, because regular smokers usually smoke the same amount over many years.
Early Morning Smoking: Lighting up a cigarette within the first 30 minutes of waking. The shorter the time to the first cigarette, the higher the degree of dependence.
Assessing the Degree of Dependence
While a clinical diagnosis of nicotine dependence is based on criteria established by psychiatric manuals, researchers and clinicians also employ self-report tests to measure its severity.
One such instrument, designed to provide a continuous and nuanced index of a smoker’s dependence, is the Cigarette Dependence Scale (CDS), developed by the author of this website and his colleagues. The shorter, 5-item version provides a quick test that can be used to tailor treatment. The longer, 12-item version (CDS-12) assessesmultiple facets of the dependence construct. By having the smoker rate statements on a five-point scale, the questionnaire provides a total score that clinicians can use to gauge the severity of the addiction, select the most appropriate treatment approach, and monitor the patient’s progress during cessation efforts.
The Biological Mechanism: Nicotine and the Brain
The invisible chain of addiction is forged in the brain’s complex circuitry. Nicotine acts as a powerful psychoactive agent, mimicking the natural neurotransmitter acetylcholine.
Upon inhalation, nicotine reaches the brain in mere seconds. There, it binds to specific protein channels, known as nicotinic acetylcholine receptors (nAChRs), located throughout the brain. When nicotine binds to these receptors, it triggers the release of several neurochemicals, most notably dopamine in the brain’s reward centers. This rush of dopamine produces the transient feelings of pleasure, focus, and reward that reinforce the act of smoking. The brain is somehow tricked to associate smoking with other rewards that are essential for survival.
With repeated exposure, the brain adapts: it produces an excess number of nAChRs in an attempt to compensate for the constant stimulation—a process called upregulation. This adaptation is the biological basis for tolerance, meaning the smoker needs more nicotine to achieve the same effect. When the nicotine supply is cut off, these upregulated receptors are left craving stimulation, leading to intense withdrawal symptoms and driving the compulsive need to smoke again. This cycle of seeking relief from discomfort is known as negative reinforcement, cementing the addiction.
The key factor is that the addictiveness of a nicotine delivery device depends on the speed at which nicotine is delivered to the blood and brain. Cigarettes have the fastest nicotine delivery, as a large amount of nicotine reaches the brain within seconds of inhaling a puff. In contrast, nicotine patches, gum, lozenges, and pouches deliver the nicotine dose much more slowly, so these products are not addictive. Electronic cigarettes and heated tobacco products have a medium delivery rate, nd some of these products can also be addictive depending on the amount and speed of nicotine delivery.
The Behavioral Component: Triggers and Rituals
Cigarette addiction is not purely chemical; it is also deeply interwoven with learned behaviors and environmental cues. This is the behavioral component of the dependence.
Smokers repeatedly link the physical act of smoking with daily routines, emotional states, and social settings. The morning coffee, the work break, driving a car, finishing a meal, talking on the phone, or experiencing stress or anxiety all become powerful cues, or “triggers,” that signal the need for a cigarette. The mere sight or smell of tobacco, or being in the presence of other smokers, can elicit a powerful craving. These ritualistic associations create a psychological dependence that must be addressed alongside the physical addiction to ensure long-term cessation.
Treatment Methods
The treatment for cigarette addiction is most effective when it is multi-faceted, addressing both the biological craving and the deeply ingrained behavioral habits, and when it combines pharmacological with behavioral treatments.
Pharmacological Treatments aim to manage the physical symptoms of withdrawal and reduce the reinforcing effects of nicotine:30
Nicotine Replacement Therapy (NRT): Available as patches, gum, lozenges, inhalers, and sprays, NRT delivers controlled doses of nicotine without the harmful toxins of tobacco smoke, and at a slower rate than cigarettes, making these products non-addictive. This helps mitigate withdrawal symptoms. Combining a long-acting form (like the patch) with a short-acting form (like the gum) for acute cravings is more effective than using either product alone.
Prescription Medications: Drugs like varenicline, cytisine and bupropion are non-nicotine options. Varenicline and cytisine work by partially stimulating the nAChR, reducing both cravings and the pleasure derived from smoking, while bupropion, originally an antidepressant, is thought to influence dopamine and norepinephrine levels to alleviate withdrawal.
Although these are not medical treatments, you can also obtain nicotine from electronic cigarettesor nicotine pouches if you do not wish to use the medications mentioned above.
Behavioral Treatments focus on disrupting the psychological and learned components of the addiction:
Cognitive Behavioral Therapy (CBT): This approach helps the smoker identify their triggers and develop effective coping strategies and relapse prevention skills. It reframes the person’s thoughts and behaviors related to smoking.
Counseling and Support: Individual or group counseling, often delivered by specialists or through telephone quitlines, provides essential support, motivation, and practical guidance on navigating the challenges of quitting.
Motivational Interviewing (MI) is a specific technique used to help ambivalent smokers explore and resolve their feelings about cessation.
Successful smoking cessation is based on a combination of medication and behavioral support tailored to your individual needs and level of dependence. Millions of people have successfully quit smoking with the help of pharmacological and behavioral aids, and you can do it too, just like them, and improve your health immediately.
Use the ‘Comments’ field below to share your experience or to suggest imporovements to this article.
References:
Etter, JF., Le Houezec, J. & Perneger, T. A Self-Administered Questionnaire to Measure Dependence on Cigarettes: The Cigarette Dependence Scale. Neuropsychopharmacol28, 359–370 (2003). https://doi.org/10.1038/sj.npp.1300030
Jean-François Etter, Comparing the validity of the Cigarette Dependence Scale and the Fagerström Test for Nicotine Dependence, Drug and Alcohol Dependence, Volume 95, Issues 1–2, 2008, Pages 152-159, ISSN 0376-8716, https://doi.org/10.1016/j.drugalcdep.2008.01.017.
Jean-François Etter, A comparison of the content-, construct- and predictive validity of the cigarette dependence scale and the Fagerström test for nicotine dependence, Drug and Alcohol Dependence, Volume 77, Issue 3, 2005, Pages 259-268, ISSN 0376-8716, https://doi.org/10.1016/j.drugalcdep.2004.08.015.